Overview of efficacy
This section presents a review of the evidence from the treatment studies that tested the effectiveness of several variants of CFBT. These studies altogether involved 339 earthquake survivors. We also used CFBT in our routine outreach care delivery to more than 6,000 survivors in Turkey, about 1,500 of whom were people who sought treatment from our community center in the disaster region. Thus, the study findings reviewed in this section were replicated in a much larger survivor population than the samples of these studies. These studies are presented in chronological sequence with a brief review of the various considerations that led to each study.
Study 1 – An open trial of Control-Focused Behavioral Treatment
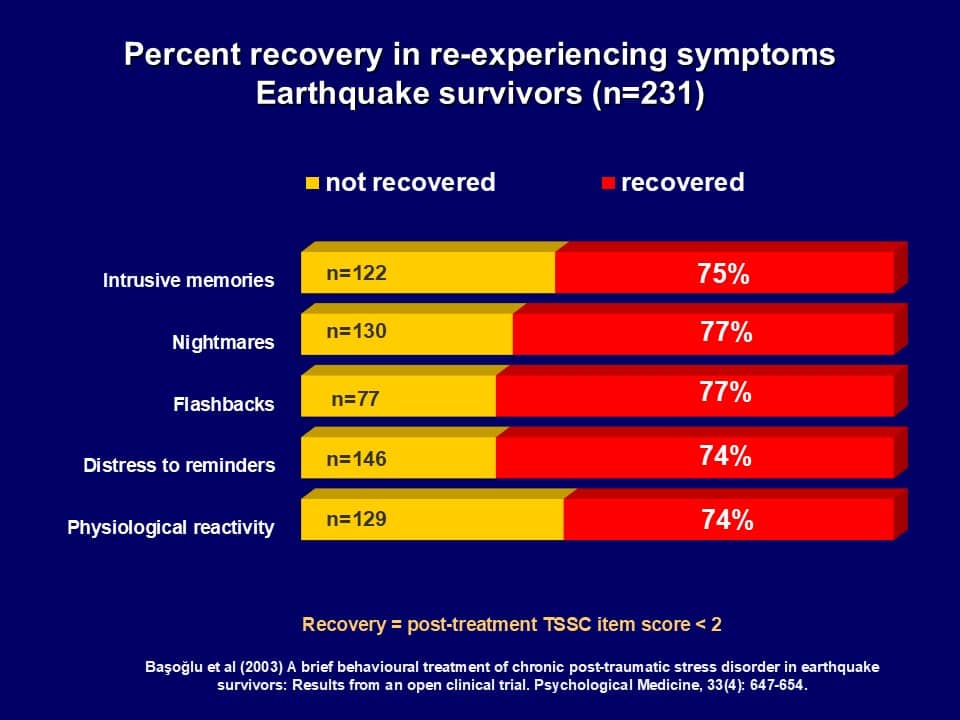
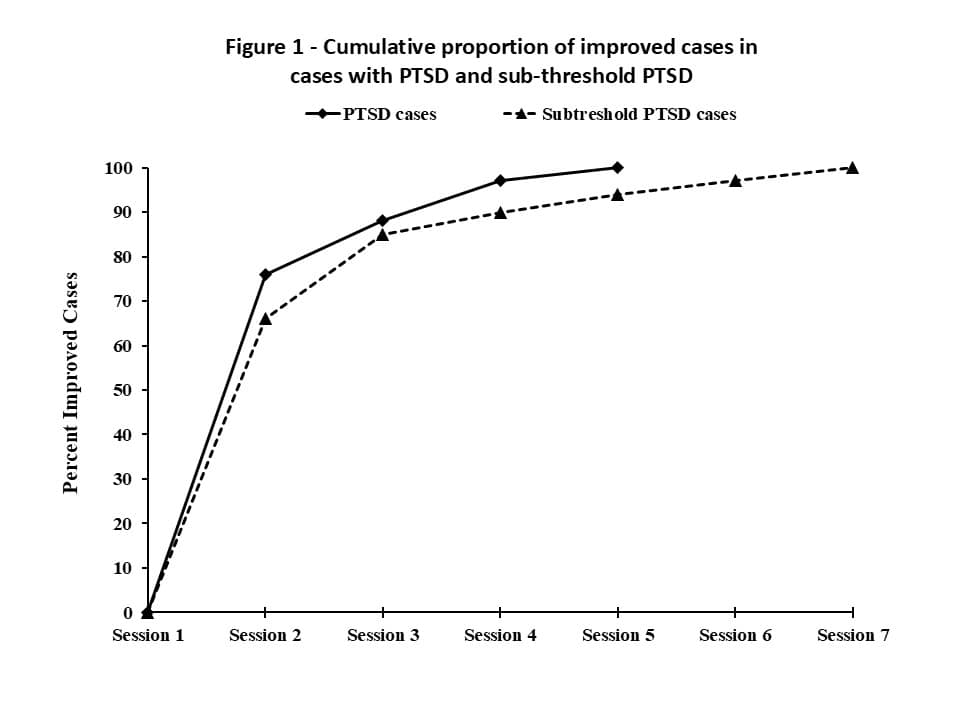 The first study that tested CFBT was an open clinical trial (Başoğlu et al., 2003b), which was launched eight months after the earthquake at a time when occasional aftershocks were still occurring. It involved 231 survivors with traumatic stress symptoms, 167 (72%) of whom had PTSD. In an effort to develop an intervention that could be delivered with as little therapist time as possible, this study was designed to examine the minimum number of sessions required for significant clinical improvement. Accordingly, treatment duration was flexible and the sessions were discontinued when significant clinical improvement occurred. The survivors were given a mean of 4.3 (SD = 2.6) treatment sessions. Exposure tasks were defined in relation to most socially disabling avoidance behaviors (e.g. staying alone at home, entering concrete buildings, etc.). The initial treatment sessions lasted about 90 minutes, while the subsequent sessions were delivered in 45 minutes. Figure 1 shows the probability of improvement after each session based on a survival analysis.
The first study that tested CFBT was an open clinical trial (Başoğlu et al., 2003b), which was launched eight months after the earthquake at a time when occasional aftershocks were still occurring. It involved 231 survivors with traumatic stress symptoms, 167 (72%) of whom had PTSD. In an effort to develop an intervention that could be delivered with as little therapist time as possible, this study was designed to examine the minimum number of sessions required for significant clinical improvement. Accordingly, treatment duration was flexible and the sessions were discontinued when significant clinical improvement occurred. The survivors were given a mean of 4.3 (SD = 2.6) treatment sessions. Exposure tasks were defined in relation to most socially disabling avoidance behaviors (e.g. staying alone at home, entering concrete buildings, etc.). The initial treatment sessions lasted about 90 minutes, while the subsequent sessions were delivered in 45 minutes. Figure 1 shows the probability of improvement after each session based on a survival analysis.
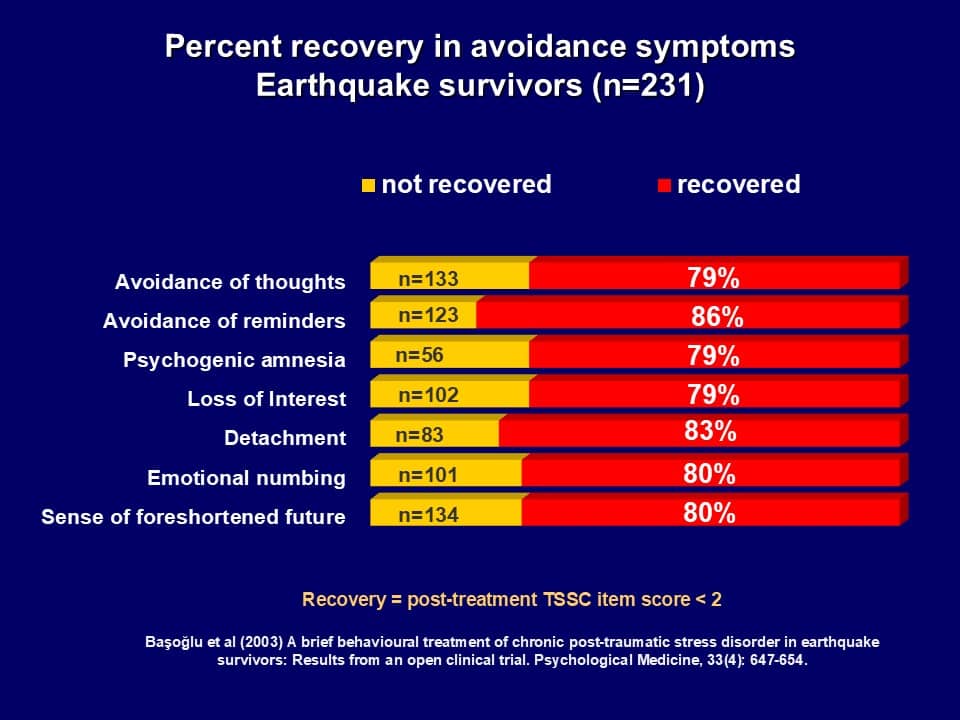
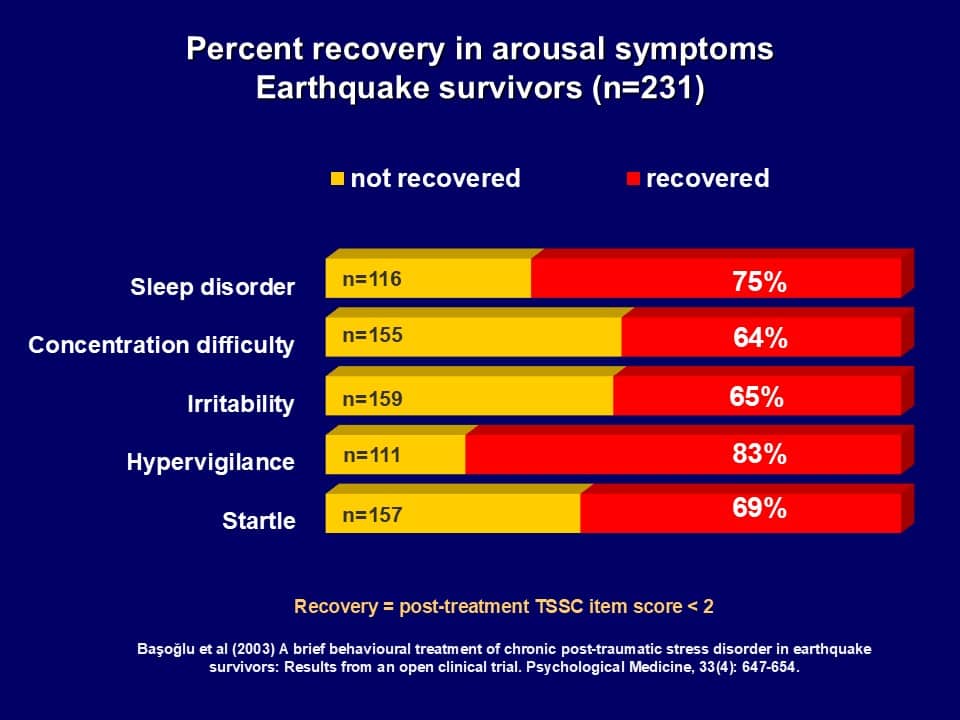
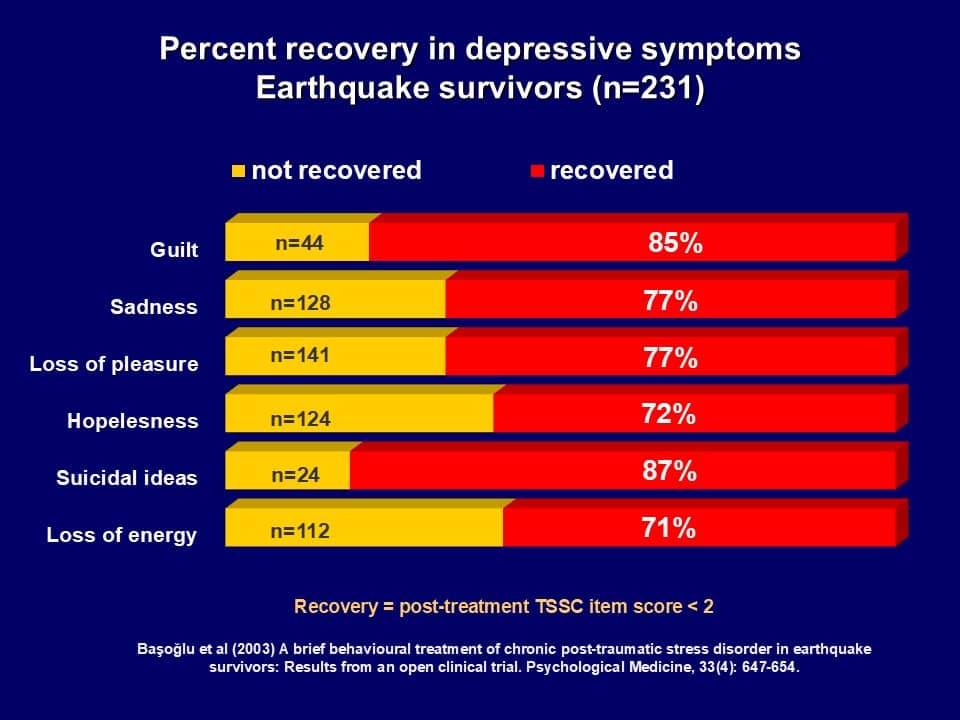
Among survivors with PTSD, the probability of improvement was 76% after one session and 88% after two sessions, reaching 100% after four sessions. Significant clinical improvement in this study corresponded to a reduction of mean 57% in PTSD symptoms, 69% in avoidance behaviors, 50% in depression symptoms, 71% in assessor-rated work and social disability. The mean number of sessions required for improvement was 1.7. All PTSD and depression symptoms improved, suggesting a ‘patholytic’ treatment effect. Improvement generalized to all PTSD and depression symptoms. Among cases where these symptoms were present at pre-treatment, the percentages of improvement (symptom rated as absent) ranged from 74% to 77% for the re-experiencing symptoms, 79% to 86% for the avoidance and numbing symptoms, 64% to 83% for the hyperarousal symptoms, and 71% to 85% for the depression symptoms (click on links to see the improvement rates on individual symptoms). It is worth noting here that improvement occurred in cognitive symptoms of PTSD and depression as well, despite the fact the treatment did not involve cognitive interventions specifically targeting these symptoms. Exposure treatment is thought to be less effective in reducing the ‘negative’ symptoms of PTSD, such as amnesia, emotional numbing, and detachment (Keane et al., 1989). Our findings did not support this view. Of particular interest was the treatment effect on psychogenic amnesia. To confirm this finding, we conducted in-depth interviews with about 10 participants of this study and found that reduction in fear and traumatic stress was indeed accompanied by significant recovery of lost memories relating to various aspects of the trauma.
No baseline variable (including severity of trauma, PTSD, and depression) predicted treatment outcome due to little variability in the outcome measures. Improvement was maintained in 74 of 75 survivors who had 3- to 9-month follow-up, despite ongoing threat to safety caused by aftershocks and expectations of another major earthquake, suggesting increased resilience against earthquake-related traumatic stress.
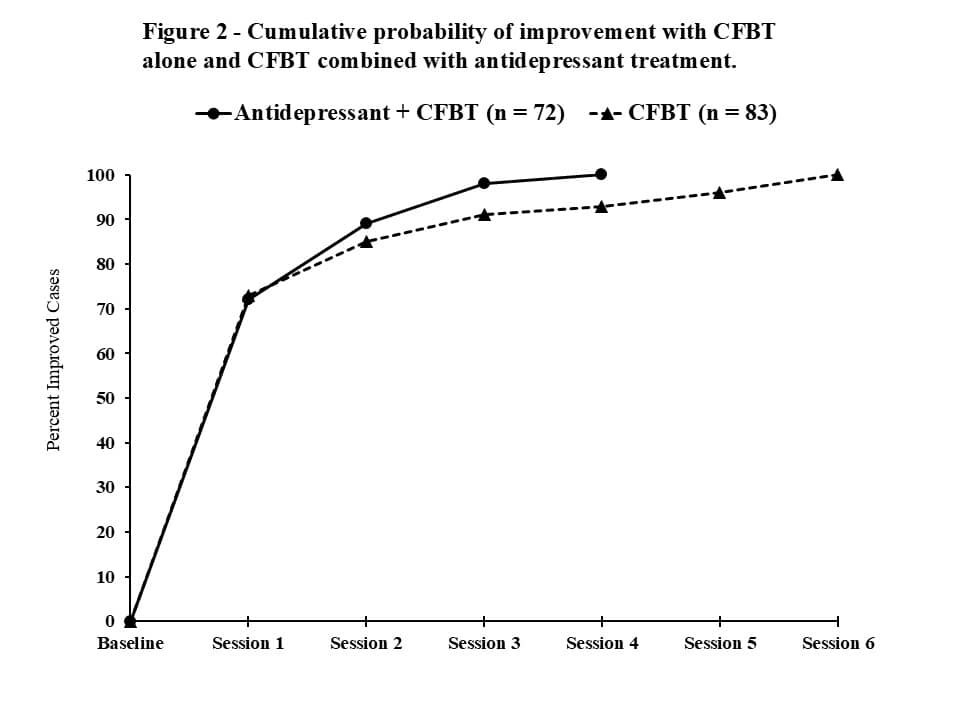 In this study 80 (35%) survivors received psychotropic drugs in addition to CFBT, including sertraline (n=43), fluoxetine (n=11), and others (n=26). Antidepressants were used only for depression with serious suicidal intent. In cases where severe depression undermined motivation for psychological treatment, CFBT was started after a few weeks of drug treatment. Care was taken to maintain a therapeutic dose for six months, whenever possible. Figure 2 shows the cumulative probability of improvement (based on a survival analysis) in survivors who received antidepressants in addition to CFBT, compared with those who received only CFBT. The analysis included only survivors that met the diagnosis of PTSD (eight excluded due to missing data).
In this study 80 (35%) survivors received psychotropic drugs in addition to CFBT, including sertraline (n=43), fluoxetine (n=11), and others (n=26). Antidepressants were used only for depression with serious suicidal intent. In cases where severe depression undermined motivation for psychological treatment, CFBT was started after a few weeks of drug treatment. Care was taken to maintain a therapeutic dose for six months, whenever possible. Figure 2 shows the cumulative probability of improvement (based on a survival analysis) in survivors who received antidepressants in addition to CFBT, compared with those who received only CFBT. The analysis included only survivors that met the diagnosis of PTSD (eight excluded due to missing data).
Figure 2 shows no substantial differences between the drug and non-drug groups in the cumulative proportion of improved cases. Additional antidepressant treatment did not speed up recovery, despite the fact that 47% of the survivors met the diagnosis of comorbid depression. This was because improvement in both PTSD and depression occurred in the CFBT only group within 3-4 weeks before the drug effect reached its maximum. Although this finding does not imply drug ineffectiveness, it suggests that antidepressant treatment is not a useful addition to CFBT, even in cases with comorbid depression, because of relatively rapid recovery achieved by CFBT.
Although this study showed that CFBT could be confidently delivered in one or two sessions, it was unclear as to whether the survivors would have improved as much after a single treatment session, if they knew that they were not going to see the therapist again for monitoring and review of progress. This was an important question, given that many survivors were not able to attend treatment more than once due to increased demographic mobility after the disaster, daily survival problems, and economic difficulties. This issue was addressed in a randomized controlled clinical trial (Başoğlu et al., 2005) of a single session of CFBT.
Study 2 – A randomized controlled trial of Single-Session CFBT
This study (Başoğlu et al, 2005b) involved 59 participants with chronic PTSD and was launched 30 months after the earthquake. The participants were recruited from among the residents of two housing sites built for homeless survivors and self-referrals to our community care center in the epicenter region. All survivors had high levels of earthquake exposure. The treatment was delivered in a single session lasting about 60 minutes. In an effort to limit the participants’ expectations from treatment to a single session, they were informed that they would receive only one treatment session and subsequent contacts would be for assessment only. Subsequent follow-up sessions were limited to assessment only (by a staff member other than the therapist) and no further self-exposure instructions were given.
Although treatment compliance was not systematically measured in this study, follow-up assessments of progress made it clear that 90% of the participants complied with self-exposure instructions. Significant treatment effects were found on all measures at post-treatment, with self-rated global improvement rates of 49% at week 6, 80% by week 12, 85% by week 24, and 83% by 1-2-year follow-up. Much of the improvement occurred during the first 12 weeks and stabilized thereafter. At the final follow-up assessment (1-2 years in most cases, last observation carried forward) fear and avoidance reduced by 69%, paralleled by 59% reduction in PTSD symptoms. All PTSD and depression symptoms showed significant improvement. As in the previous study, the relapse rate was very low, with only one survivor losing treatment gains during follow-up. This study showed that CFBT could be effectively delivered in a single session, without the usual monitoring component of traditional behavior therapy (e.g. reinforcement, verbal praise, troubleshooting, diary-keeping, setting of new homework exposure tasks, etc.).
In our review of the learning theory model of traumatic stress we had hypothesized that ‘risk-taking’ behaviors, such as not avoiding feared situations, reduce helplessness responses, thereby leading to recovery from traumatic stress (Başoğlu et al, 2011). This formulation implied a certain sequence of events during the improvement process. If the intervention (e.g. treatment rationale and encouragement for risk taking behaviors) enhance sense of control over fear, then the first change event one would expect early in treatment is reduced behavioral avoidance of feared situations. Second, if there is an association between reduced behavioral avoidance (which implies increased sense of control), then one would expect a generalized effect of reduced avoidance on all other traumatic stress responses, including PTSD and depression. We tested these hypotheses by examining which symptoms improved first early in treatment (Şalcıoğlu, Başoğlu, & Livanou, 2007). Among all PTSD symptoms, behavioral avoidance as the only symptom that showed a significant between-group treatment effect at week 6. Significant improvement in the other PTSD symptoms appeared at subsequent follow-up assessments, reaching a maximum at week 24. Recovery rates (symptom absent) at week 24 ranged from 60% to 89% for most PTSD symptoms, indicating generalized improvement. Compared to those who recovered from behavioral avoidance, those who still had the symptom at week 24 were more likely to have intrusive memories, nightmares, distress upon reminders, physiological reactivity, avoidance of trauma-related thoughts, loss of interest, hypervigilance, startle, insomnia, memory and concentration difficulty, emotional numbing, and detachment. Thus, improvement in 12 PTSD symptoms was associated with improvement in avoidance. Compared to avoidant survivors, those who recovered from avoidance showed twice as much reduction in total Clinician-Administered PTSD Scale (CAPS; Blake et al., 1990) scores (excluding behavioral and cognitive avoidance symptoms). These findings clearly supported the critical role of reduced behavioral avoidance in recovery from helplessness and associated traumatic stress responses. Although helplessness responses (or sense of control over fear) were not directly measured in this study, the strong associations among fear, avoidance, helplessness, and hopelessness responses documented in Başoğlu et al, 2011 suggest that reduced avoidance most probably indicated enhanced sense of control over fear in this study. This is also supported by the fact that depressive symptoms as measured by Beck Depression Inventory (Beck et al., 1979) reduced by 51% at week 24. The possible role of increased sense of control in improvement with CFBT will be discussed further later in this section.
Study 3 – An experiment with Earthquake Simulation Treatment
 Although the first two studies found high rates of global improvement with one or two sessions of CFBT, the extent of reduction in PTSD symptoms was about 60% in both studies, suggesting that the survivors still had some residual symptoms. Furthermore, in the second study, participants with more severe fear, PTSD, depression, and social disability improved less, mainly because of their difficulty in conducting self-exposure. Thus, it appeared that the intervention fell short of providing sufficient encouragement for self-exposure in survivors with initially higher levels of illness severity. In a further effort to maximize the effectiveness of the behavioral treatment program, an experiment was conducted with 10 survivors who had PTSD according to CAPS to examine whether exposure to simulated earthquake tremors (Earthquake Simulation Treatment) would enhance sense of control over fear and thereby facilitate subsequent self-exposure to fear cues (Başoğlu et al., 2003a). This experiment was inspired by our observations of panic responses in survivors to earthquake-like shaking or ground vibrations, such as those created by passing trucks in locations close to highways. In addition, we had observed that people with previous experience of such shaking movements (e.g. sailors) showed less fear responses to aftershocks and more rapid reduction in fear with repeated exposures to aftershocks. These findings suggested that simulated unconditioned stimuli (i.e. earthquake tremors) could be used as fear cues in exposure treatment to enhance sense of control over real earthquake tremors.
Although the first two studies found high rates of global improvement with one or two sessions of CFBT, the extent of reduction in PTSD symptoms was about 60% in both studies, suggesting that the survivors still had some residual symptoms. Furthermore, in the second study, participants with more severe fear, PTSD, depression, and social disability improved less, mainly because of their difficulty in conducting self-exposure. Thus, it appeared that the intervention fell short of providing sufficient encouragement for self-exposure in survivors with initially higher levels of illness severity. In a further effort to maximize the effectiveness of the behavioral treatment program, an experiment was conducted with 10 survivors who had PTSD according to CAPS to examine whether exposure to simulated earthquake tremors (Earthquake Simulation Treatment) would enhance sense of control over fear and thereby facilitate subsequent self-exposure to fear cues (Başoğlu et al., 2003a). This experiment was inspired by our observations of panic responses in survivors to earthquake-like shaking or ground vibrations, such as those created by passing trucks in locations close to highways. In addition, we had observed that people with previous experience of such shaking movements (e.g. sailors) showed less fear responses to aftershocks and more rapid reduction in fear with repeated exposures to aftershocks. These findings suggested that simulated unconditioned stimuli (i.e. earthquake tremors) could be used as fear cues in exposure treatment to enhance sense of control over real earthquake tremors.
Earthquake Simulation Treatment
 Earthquake Simulation Treatment (EST) is designed to help an earthquake survivor gain sense of control over earthquake tremors using an earthquake simulator. It is an innovative treatment designed by Professor Başoğlu to enhance the potency of CFBT even further by helping survivors develop a sense of control over earthquake tremors and used for the first time in Turkey. The earthquake simulator is specifically designed for treatment purposes. It is a small furnished house based on a shake table that simulates earthquake tremors up to 8 magnitude on a Richter scale. A computer executes the movements of the simulator in accordance with various preprogrammed earthquake scenarios.
Earthquake Simulation Treatment (EST) is designed to help an earthquake survivor gain sense of control over earthquake tremors using an earthquake simulator. It is an innovative treatment designed by Professor Başoğlu to enhance the potency of CFBT even further by helping survivors develop a sense of control over earthquake tremors and used for the first time in Turkey. The earthquake simulator is specifically designed for treatment purposes. It is a small furnished house based on a shake table that simulates earthquake tremors up to 8 magnitude on a Richter scale. A computer executes the movements of the simulator in accordance with various preprogrammed earthquake scenarios.
The users can control the tremors from the inside using a mobile control switch, stopping or starting it anytime they want and increasing the intensity whenever they feel ready for it. Being in complete control of the tremors enables users to keep their distress or anxiety within manageable levels. The experience often evokes two types of emotions: fear associated with the tremors and distress related to memories of the traumatic events during the earthquake. This allows opportunities for the users to exercise and gain control over both types of emotions. The session is terminated when the users feel in complete control of their distress or fear. In almost all cases the experience leads to a substantial reduction in these emotions.
An imaginative depiction of Earthquake Simulation Treatment – Courtesy of José Carlos Fernandes – a Portuguese artist
In the pilot study, the sessions lasted one hour, starting with the lowest intensity level and going one level up as the survivor gained sense of control over the tremors. About 80% of the treatment session time was spent at the lowest intensity levels (corresponding to approximately 3- to 4-magnitude tremors on the Richter scale). Treatment was terminated when the survivor felt in control of his / her anxiety or distress. After the session, no specific self-exposure instructions were given so that the effect of the treatment session alone on sense of control could be examined in the long-term. It was hypothesized that the intervention alone (without therapist encouragement and instructions for self-exposure to feared situations) would achieve sufficient increase in sense of control, thereby reducing behavioral avoidance of earthquake reminders and other traumatic stress reactions.
Assessment immediately after session termination revealed substantial reduction in anticipatory fear of earthquakes and distress associated with trauma memories. Assessments at weeks 2, 4, 8, and 12 showed a steady decrease in avoidance of feared situations, resulting in 66% reduction in total Fear an Avoidance Questionnaire (FAQ) scores at the last follow-up. This was paralleled by 71% reduction in PTSD and 66% reduction in depression symptoms. Eight survivors were markedly and two slightly improved at week 12.
These findings were important in suggesting that exposure to simulated earthquake tremors was highly effective in reducing behavioral avoidance. Two points deserve attention here. First, the study participants were told that the treatment involves a single session of exposure to simulated earthquake tremors to help them overcome their fear of earthquakes and resume their normal life. They were not given instructions or any encouragement for self-exposure after the session. The therapist refrained from even mentioning the idea. Nonetheless, the survivors subsequently instigated self-exposure with a steady decrease in their avoidance behaviors. Such sequence of events points to the possible role of increased sense of control over fear at post-session. A greater reduction in PTSD symptoms than in the previous two studies also attested to the potency of the intervention. This implied that adding a component of live exposure to single-session CFBT was likely to enhance the effectiveness of the latter, particularly in survivors with difficulty in initiating self-exposure.
Study 4 – A randomized controlled trial of Earthquake Simulation Treatment
The effectiveness of a combined approach using a single session of exposure to simulated earthquake tremors and self-exposure instructions was examined in a randomized controlled study (Başoğlu et al., 2007) involving 31 survivors with chronic PTSD. The study sample was drawn from the same population of earthquake survivors with high trauma exposure as in the previous studies. The study was launched about four years after the earthquake. Between-group treatment effects were examined at week 8, after which the control group was crossed over to receive the same treatment.
Treatment was delivered in two steps. At the first step the treatment and its rationale were explained, exposure tasks were defined, and self-exposure instructions were given. The second step involved Earthquake Simulation Treatment. The participants were informed that this intervention was designed to enhance their sense of control over earthquake tremors and also to demonstrate to them how they can overcome their fears. The session was conducted in the same way described earlier (mean session duration 33 minutes, SD = 18, range 9-70 minutes).
Assessment at post-session indicated that 30 of the 31 participants rated the session as fairly to very similar to their experience of the 17th of August earthquake. This finding is of interest because 29 of the participants experienced simulated tremors at levels lower than 4, which corresponded to a magnitude of about 6 on the Richter scale. Nevertheless, most survivors found the tremors very similar to the 17th of August earthquake, which had a magnitude of 7.4. We had originally thought that the magnitude of the simulated earthquake was likely to be a critical factor in perceived similarity to the original earthquake experience (and thus in improvement) but we were wrong. Higher tremor magnitudes were required in only two survivors, who did not experience significant distress at levels lower than 4.
Thirty participants found the experience fairly to very much useful and felt satisfied with the treatment. Eighteen (72%) participants reported marked to very much reduction in their anticipatory fear of future earthquakes. The treatment effects at week 8 were significant on all measures of fear, PTSD, depression, and self- and assessor-rated global improvement. Clinically significant improvement rates (Jacobson & Truax, 1991) were 52% at week 4, 72% at week 12, 92% at week 24, and 92% at 1-2-year follow-up. Among the improved cases at week 12, only one showed relapse during further follow-up.
In this study treatment effect on sense of control was measured by a Sense of Control Scale (SCS) with five items tapping change in fears, sense of control over feared situations, and courage, self-confidence, and belief about ability to cope in feared situations, each rated on a 0–3 scale (0 = no change or worsening, 3 = much increased/decreased). The mean SCS scores (range 0 – 15) ranged from 8.3 (SD = 3.6) at week 4 to 11 (SD = 4.1) at 1-2 year follow-up, indicating marked to much increase in sense of control over fears. The SCS correlated significantly with reduction in CAPS scores at all follow-up assessments, thus evidencing an association between increased sense of control and improvement in PTSD. Increased sense of control also meant enhanced resilience, as suggested by the fact that 11 of the 13 survivors who experienced an earthquake sometime after the treatment reported much less fear than usual during the tremors.
A meta-analytic comparison of studies of CFBT in earthquake survivors
Table 1 shows a comparison of findings across the four studies in terms of within-group effect sizes. As two of the studies did not involve controls, a comparison in between-group effect sizes was not possible.
| Table 1 – Effect Sizes in Clinical trials of Control-Focused Behavioral Treatmenta | ||||
| Study 1b
(n = 143) |
Study 2c
(n = 51) |
Study 3d
(n = 10) |
Study 4e
(n = 25) |
|
| Clinician Administered PTSD Scale | — | 1.80 | 2.58 | 3.51 |
| Traumatic Stress Symptom Checklist | 1.92 | 1.95 | 2.59 | — |
| Fear and Avoidance Questionnaire | 1.97 | 1.90 | 2.07 | 2.29 |
| Beck Depression Inventory | 1.22 | 1.13 | 1.56 | 2.47 |
| Work and Social Adjustment –Assessor | 1.84 | — | — | 2.91 |
| Work and Social Adjustment -Self | 1.35 | 1.19 | — | — |
| a Cohen’s d at last assessment available / b Self-exposure instructions (mean 4.3 sessions). Analyses based only on cases with PTSD to allow comparison with the other studies / c Single-session CFBT involving self-exposure instructions / d Single session of Earthquake Simulation Treatment / e Single-session CFBT combined with Earthquake Simulation Treatment | ||||
In all studies, treatment had a patholytic effect on all problem areas (including impairment in work, social, and family functioning) reducing not only fear and PTSD but also depression. The effect sizes on the PTSD measures were larger in the studies involving Earthquake Simulation Treatment than in studies of self-exposure alone. Compared with self-exposure instructions alone, combined treatment achieved greater reduction in PTSD (59% vs. 79%, respectively) and better end-state functioning, with greater improvement in symptoms of irritability, loss of interest, nightmares, distress related to trauma reminders, emotional numbing, sense of foreshortened future, sleeping difficulty, and memory / concentration difficulty (Başoğlu et al., 2007). Unlike in Study 2, pre-treatment illness severity did not predict treatment outcome, suggesting enhanced treatment effects in cases with high pre-treatment anxiety.
Study 5 – Treatment studies with children
 The effectiveness of CFBT in children was tested in a pilot study (Şalcıoğlu & Başoğlu, 2008) involving 23 school age children with PTSD at 20 months post-disaster. Treatment was delivered twice-weekly in groups across 6 sessions after a variable waiting period ranging from 1 to 18 weeks. While no significant improvement was found during the waiting period, the children showed 50% reduction in PTSD and 55% reduction in earthquake-related fears at post-treatment. These findings suggested that CFBT has promise in treatment of child earthquake survivors. This is not surprising, given that earthquake-induced PTSD in children is mediated by the same process as in adults, i.e. loss of control over fear. Thus, encouraging children to overcome their fear through self-exposure facilitates their recovery from posttraumatic stress. Children relate very well to the rationale of the treatment (e.g. ‘you’re your fear’) and generally display greater compliance with self-exposure instructions than do adults.
The effectiveness of CFBT in children was tested in a pilot study (Şalcıoğlu & Başoğlu, 2008) involving 23 school age children with PTSD at 20 months post-disaster. Treatment was delivered twice-weekly in groups across 6 sessions after a variable waiting period ranging from 1 to 18 weeks. While no significant improvement was found during the waiting period, the children showed 50% reduction in PTSD and 55% reduction in earthquake-related fears at post-treatment. These findings suggested that CFBT has promise in treatment of child earthquake survivors. This is not surprising, given that earthquake-induced PTSD in children is mediated by the same process as in adults, i.e. loss of control over fear. Thus, encouraging children to overcome their fear through self-exposure facilitates their recovery from posttraumatic stress. Children relate very well to the rationale of the treatment (e.g. ‘you’re your fear’) and generally display greater compliance with self-exposure instructions than do adults.
The therapeutic effects of exposure to feared situations in children were indeed observed in another pilot study (Şalcıoğlu & Başoğlu, 2008) involving Earthquake Simulation Treatment. This study involved a series of 8 multiple-baseline experimental case studies with 4 boys and 4 girls (aged 8 to 13) treated in the same session. While no significant improvement was noted during an initial 2 to 5 weeks of waiting period, both fear and PTSD symptoms showed 52% reduction at 1-2-month post-treatment follow-up. On a self-rated global improvement measure, 5 children (63%) reported much / very much improvement, 2 slight improvement and 1 no change. Parental assessment indicated similar improvement in school and family functioning.
Study 6 – A study of CFBT of war and torture survivors
This study was conducted to examine the minimum number of treatment sessions needed to achieve significant clinical improvement in war and torture survivors. It involved 80 asylum-seekers referred to the project by various refugee care agencies in Istanbul. Of these, 20 were lost to the study for various reasons (mostly unrelated to treatment response), so the results were based on 60 cases. The study was conducted as part of routine care of asylum-seekers referred to the project. Among all referrals, cases with PTSD were consecutively included in the study. Only psychotic cases were excluded.
Of the 60 study completers, 47% were from Democratic Republic of Congo, 18% from other African countries, 27% from Iraq, and 8% from other Middle Eastern and Asian countries. The most commonly reported trauma experiences were witnessing war atrocities, exposure to bombings, sexual violence including gang rape (37%), and torture (32%). In most tortured cases, torture had been perpetrated by non-state actors (e.g., rebel groups, paramilitaries, etc.). Fifty-seven percent of the cases were female, and the mean age was 25 (SD 10). Forty-seven percent were illiterate, or literate with no schooling, or had only primary school education. None of the study participants were on any medication for traumatic stress problems and no psychotropic drugs were used in treatment.
The study did not include a control group, but the non-specific effects of therapist contact and pre-treatment assessment were examined in a subset of 25 cases by using a single-case multiple baseline experimental design. This included two baseline assessments conducted three weeks apart with no treatment in the interim period. Treatment was initiated after the second baseline assessment. The mean CAPS scores showed no reduction at the second baseline, meaning that therapist contact had no effect on PTSD symptoms. This suggests that the improvement in PTSD symptoms at post-treatment can be attributed to the specific effects of treatment.
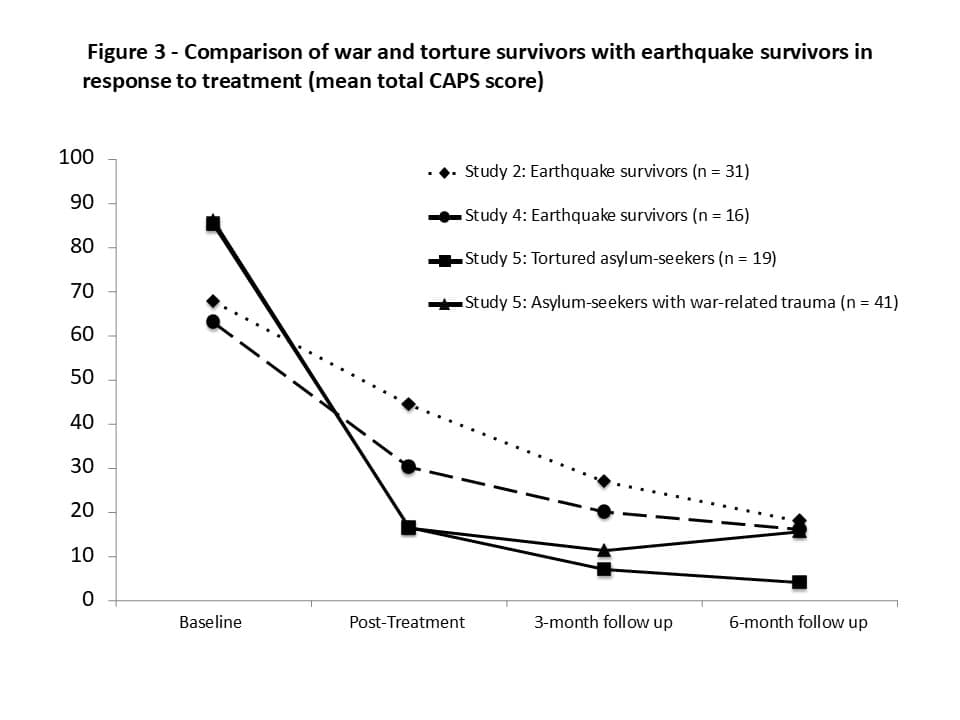 Because the main aim of this study was to examine the minimum number of treatment sessions required for significant clinical improvement, treatment duration was flexible and involved a maximum of 12 sessions. Treatment was terminated (and follow-up phase initiated) when a rating of ‘much / very much improved’ was obtained on Patient’s Global Improvement (PGI), a 1-7 scale used to assess overall clinical improvement (1 = very much improved, 2 = much improved, 3 = slightly improved, 4 = no change, 5 = slightly worse, 6 = much worse, 7 = very much worse). Our studies have shown that this is valid and reliable measure of overall clinical improvement. As it reflects patients’ own assessment of improvement, it is free from assessor bias. Depression was assessed by using Beck Depression Inventory (BDI; Beck et al, 1974). Treatment effects on PTSD and depression are shown in Figure 3 and Figure 4, respectively.
Because the main aim of this study was to examine the minimum number of treatment sessions required for significant clinical improvement, treatment duration was flexible and involved a maximum of 12 sessions. Treatment was terminated (and follow-up phase initiated) when a rating of ‘much / very much improved’ was obtained on Patient’s Global Improvement (PGI), a 1-7 scale used to assess overall clinical improvement (1 = very much improved, 2 = much improved, 3 = slightly improved, 4 = no change, 5 = slightly worse, 6 = much worse, 7 = very much worse). Our studies have shown that this is valid and reliable measure of overall clinical improvement. As it reflects patients’ own assessment of improvement, it is free from assessor bias. Depression was assessed by using Beck Depression Inventory (BDI; Beck et al, 1974). Treatment effects on PTSD and depression are shown in Figure 3 and Figure 4, respectively.
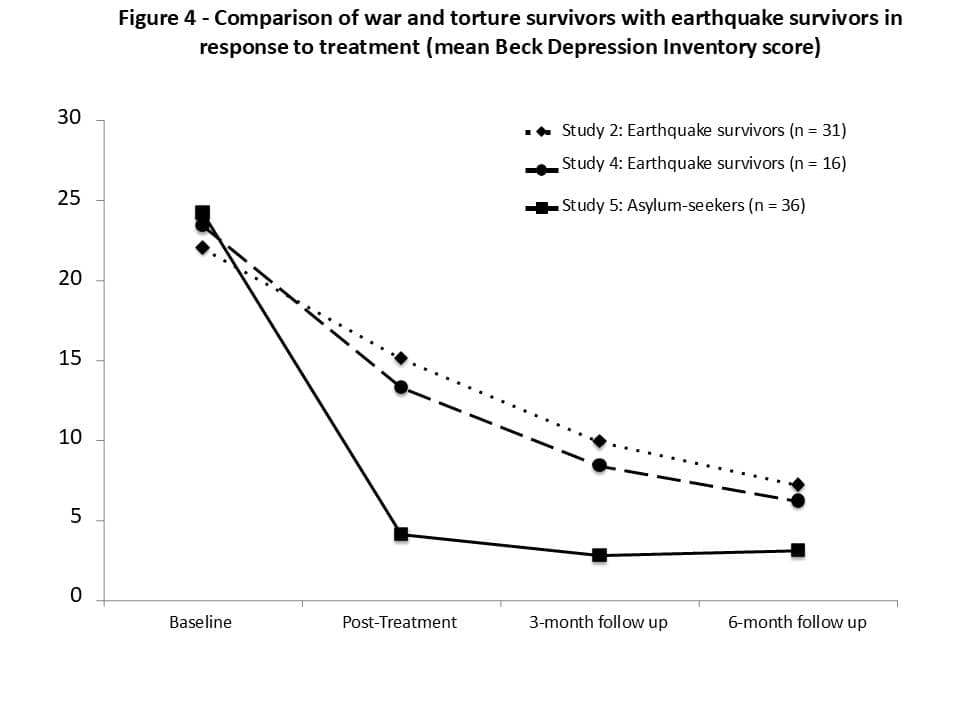 The results are shown together with the results of two randomized controlled studies of single-session CFBT in earthquake survivors (Study 2 and Study 4) to demonstrate the effectiveness of the treatment in different trauma groups and how the outcomes of a single treatment session compare with those of full-course CFBT. Figure 3 shows outcome separately for asylum-seekers with and without torture experience (difference non-significant), whereas Figure 4 shows outcome in pooled subgroups (which also showed no significant difference). Also, depression was assessed in only 36 refugees due to unavailability of BDI in some languages.
The results are shown together with the results of two randomized controlled studies of single-session CFBT in earthquake survivors (Study 2 and Study 4) to demonstrate the effectiveness of the treatment in different trauma groups and how the outcomes of a single treatment session compare with those of full-course CFBT. Figure 3 shows outcome separately for asylum-seekers with and without torture experience (difference non-significant), whereas Figure 4 shows outcome in pooled subgroups (which also showed no significant difference). Also, depression was assessed in only 36 refugees due to unavailability of BDI in some languages.
In study 2 and Study 4 the waitlist control group cases were crossed over after post-treatment assessment to receive active treatment following the same study design. In both studies the two groups were pooled together to examine the long-term global improvement rates in larger samples. Global improvement rates in Study 2 were 80% at 3-month follow-up, 85% at 6-month follow-up, and 83% at 1-2-year follow-up. The respective figures were 72%, 80%, and 80% in Study 4. The improvement rates at 6-month follow-up in the two studies correspond to within-group effect sizes of 1.6 and 3.5, respectively (mean 2.55).
In study 5 the mean number of sessions required for much / very much improvement in the sample was 6, which corresponded to the 7th week in treatment. The maximum number of sessions required for improvement was 3 or 4 in 20% of the cases, 5 to 6 in 35%, 7 to 10 in 25%, and 12 in only 5%. Of the 60 cases, 56 (93%) met the criterion of much / very much improved at some point during treatment, which corresponded to 82% reduction in PTSD symptoms (81% in tortured cases and 82% in non-tortured cases). Although four cases rated themselves as ‘slightly improved,’ their PTSD symptoms showed mean 71% improvement. The CAPS score at post-treatment was under 20 in 70% of the cases (indicating near-complete recovery), between 20 and 39 (mild / sub-threshold PTSD) in 27%, and between 40-59 (moderately severe PTSD) in only 2 (3%) cases. Thus, 97% of the cases were either nearly asymptomatic or had only mild PTSD symptoms at the end of treatment. This outcome measure based on CAPS score is used in clinical studies to assess the end-state functioning achieved by treatment. It correlates highly with recovery from the disabling effects of trauma on social, occupational, and family functioning.
The mean pre-treatment CAPS score among the asylum-seekers was 85, which indicates extremely severe PTSD, compared with 68 in Study 2 and 63 in Study 4, both of which fall into the category of severe PTSD. Despite such high levels of illness severity, the asylum-seekers showed greater improvement in both PTSD and depression than did earthquake survivors at post-treatment. This finding probably reflects the fact that the treatment was delivered to earthquake survivors in a single session, whereas the refugees received full-course CFBT. Note, however, that the improvement trends in the three groups converge at 6-month follow-up, suggesting that improvement with a single treatment session is slower but runs a steady course over 6 months, reaching the same level of improvement achieved by full-course treatment. This finding implies that CFBT can be administered on a largely self-help basis in war and torture survivors. Because Study 5 aimed at examining the optimum number of treatment sessions required for much / very much improvement, treatment had to be continued until such improvement occurred. It could have been discontinued earlier, as soon as the survivors showed sufficient reduction in avoidance behaviors (e.g., by 20%), thereby reaching a stage in treatment beyond which they might have been capable of conducting exposure on their own. Viewed together with the outcomes of a single-session CFBT in earthquake trauma, this possibility raises the prospect of a treatment even briefer than 6 sessions, possibly involving 1 to 3 sessions. Furthermore, CFBT could be helpful in reducing traumatic stress in some cases even when delivered on a solely self-help basis (e.g., through self-help tools). There is indeed preliminary evidence from a pilot study (Başoğlu et al, 2009) with earthquake survivors showing that treatment delivered by a structured self-help manual can achieve a similar improvement rate as therapist-delivered treatment. This hypothesis is well worth testing in future research with war and torture survivors.
References
Başoğlu, M., Livanou, M. & Şalcıoğlu, E. (2003a). A single session with an earthquake simulator for traumatic stress in earthquake survivors. American Journal of Psychiatry, 160, 788-790.
Başoğlu, M., Livanou, M., Şalcıoğlu, E. & Kalender, D. (2003b). A brief behavioural treatment of chronic post-traumatic stress disorder in earthquake survivors: results from an open clinical trial. Psychological Medicine, 33, 647-654.
Başoğlu, M. & Şalcıoğlu, E. 2011) A Mental Healthcare Model for Mass Trauma Survivors: Control-Focused Behavioral Treatment of Earthquake, War, and Torture Trauma. Cambridge University Press.
Başoğlu, M., Livanou, M. & Şalcıoğlu, E. (2003a). A single session with an earthquake simulator for traumatic stress in earthquake survivors. American Journal of Psychiatry, 160, 788-790.
Başoğlu, M., Livanou, M., Şalcıoğlu, E. & Kalender, D. (2003b). A brief behavioural treatment of chronic post-traumatic stress disorder in earthquake survivors: results from an open clinical trial. Psychological Medicine, 33, 647-654.
Başoğlu, M., Şalcıoğlu, E. & Livanou, M. (2007). A randomized controlled study of single-session behavioural treatment of earthquake-related post-traumatic stress disorder using an earthquake simulator. Psychological Medicine, 37, 203-213.
Başoğlu, M., Şalcıoğlu, E. & Livanou, M. (2009). Single-case experimental studies of a self-help manual for traumatic stress in earthquake survivors. Journal of Behavior Therapy and Experimental Psychiatry 40, 50-58.
Başoğlu, M., Şalcıoğlu, E., Livanou, M., Kalender, D. & Acar, G. (2005b). Single-session behavioral treatment of earthquake-related posttraumatic stress disorder: A randomized waiting list controlled trial. Journal of Traumatic Stress, 18, 1-11.
Beck, A. T., Rush, A. J., Shaw, B. F. & Emery, G. (1979). Cognitive Therapy of Depression, New York: Guilford Press.
Beck, A. T., Rial, W. Y., & Rickels, R. (1974) Short form of depression inventory: cross validation.
Psychological Reports, 34, 1184 –1186.
Blake, D. D., Weathers, F. W., Nagy, L. M., Kaloupek, D. G., Charney, D. S. & Keane, T. M. (1990). Clinician-Administered PTSD Scale (CAPS) – Current and Lifetime Diagnostic Version, Boston: National Center for Posttraumatic Stress Disorder, Behavioral Science Division.

{kind=link}
{kind=link}
{kind=link}
{kind=link}