Distinctive features
 Given that CFBT relies heavily on exposure in reducing trauma-induced helplessness, the reader might wonder whether it is a new treatment or simply a variant of exposure therapy. Although the differences of CFBT from traditional habituation-based exposure treatment are evident from its description in Başoğlu et al (2011), a more focused overview of this issue here might be helpful, particularly for readers with less experience with behavioral treatment.
Given that CFBT relies heavily on exposure in reducing trauma-induced helplessness, the reader might wonder whether it is a new treatment or simply a variant of exposure therapy. Although the differences of CFBT from traditional habituation-based exposure treatment are evident from its description in Başoğlu et al (2011), a more focused overview of this issue here might be helpful, particularly for readers with less experience with behavioral treatment.
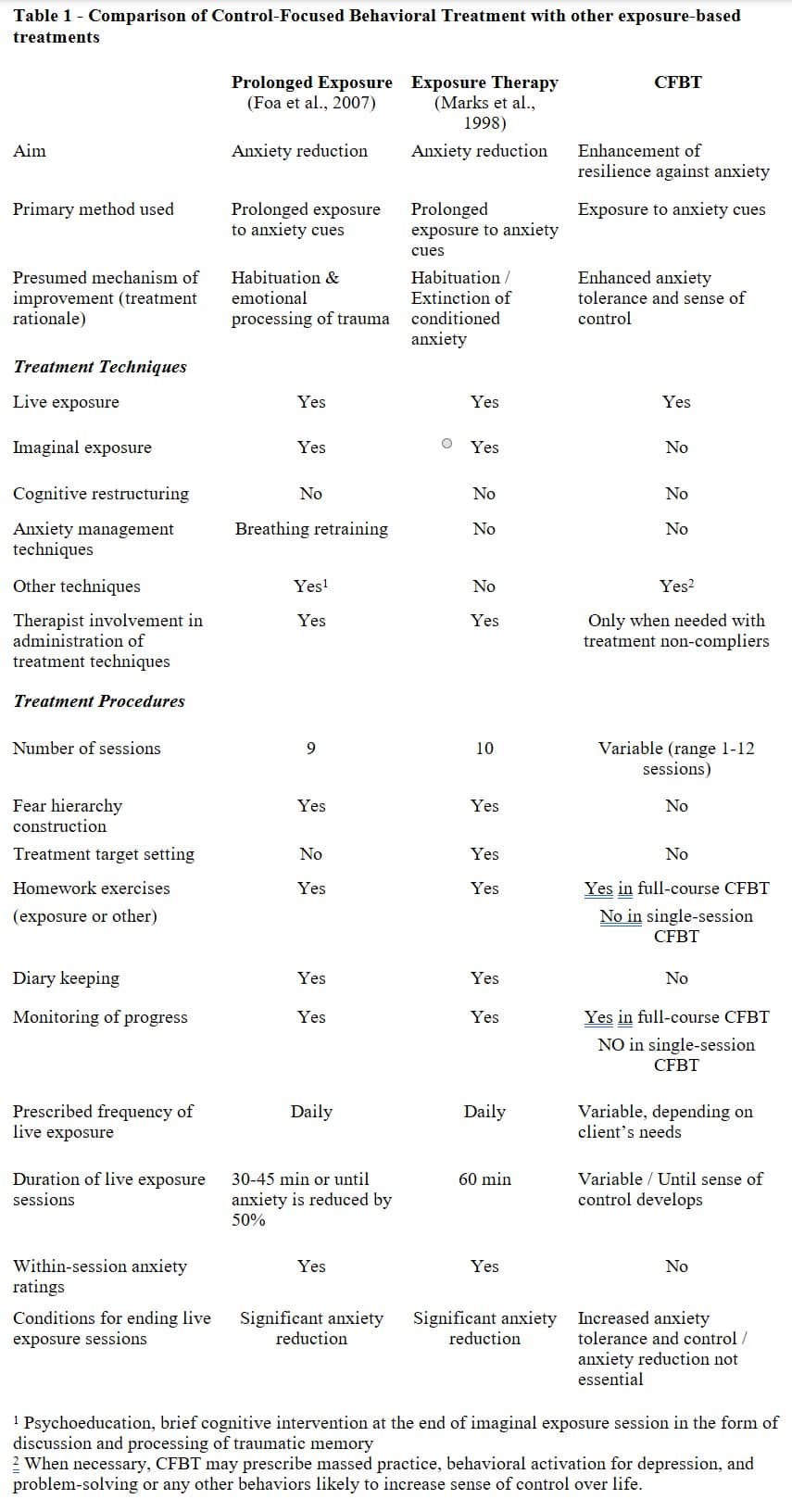
It is reasonable to argue that a treatment for a given problem is distinct from other interventions to the extent that it is different in its underlying theory, aims, mechanisms of action, and techniques and procedures. Table 1 provides a comparison between CFBT and two well-known examples of exposure treatment with respect to these features. These are prolonged exposure by Foa and colleagues (2007) and exposure treatment by Marks and colleagues (1998). The details of exposure treatments have been obtained from these authors’ treatment protocols. As CFBT is readily distinguishable from cognitive treatments (e.g. those used by Ehlers et al., 2005 and Resick & Schnicke, 1993) in not involving cognitive restructuring, the latter treatments are not included in Table 1 for comparison. Nonetheless, much of the following discussion also applies to these treatments.
Aim in treatment: Resilience building
CFBT fundamentally differs from both cognitive and exposure treatments in its primary objective. While the latter aim to reduce anxiety, CFBT is designed to enhance sense of control over anxiety, which we refer to as resilience. Resilience is a multifaceted concept that is challenging to define and operationalize. We approached this idea from a learning theory perspective (Başoğlu & Mineka, 1992), defining it as
“the capacity to exert sufficient control over stressful events by employing cognitive and/or behavioral strategies to either prevent the stressor, or, if unavoidable, take reasonable steps to protect oneself from its harmful effects, use strategies to reduce associated distress, or simply endure or tolerate it without losing control.”
In our studies with torture survivors (Başoğlu et al., 1994, 1997), we operationalized this definition of resilience by developing a “Psychological Preparedness for Torture Scale.” This scale consisted of seven items with well-defined anchor points: (1) preparedness for arrest and torture (assessed through the survivor’s political views, commitment to a cause, willingness to accept the consequences of their actions, and any prior training in physical and mental stoicism as part of political group activities), (2) political activity prior to captivity, (3) prior knowledge about torture events, (4) threat of arrest or torture prior to captivity, (5) commitment to a political cause, (6) commitment to a political group, and (7) predictability of arrest or torture. These items, reflecting pre-torture experiences that enhance resilience, demonstrated strong predictive validity regarding the psychological status of survivors after their torture experiences. Assessed an average of 61 months after their last torture, 55 political activists—who reported an average of 291 exposures to 23 forms of torture over a mean captivity period of 47 months—showed remarkably low rates of moderately severe PTSD (18%) and major depression (2%). In contrast, non-activist torture survivors, despite experiencing much less severe torture, had substantially higher rates of PTSD (58%) and depression (24%). Psychological preparedness emerged as the strongest predictor of PTSD, underscoring the critical role of perceived control and resilience in mitigating the long-term psychological impact of extreme adversity.
Such remarkable resilience against torture can be explained by prior experiences of political activists that enable them to exercise effective control strategies to secure safety (e.g. by removing or warding off threat), reduce the impact of the event if it cannot be avoided, and gain control over fear evoked by the stressor. Effective control is often achieved on cognitive, behavioral, or emotional levels. Such control often reduces anxiety or fear during exposure to the stressor event, facilitates recovery from the acute impact of trauma, and reinforces expectations of control over future stressor events. Achieving effective control over stressor events is known to have protective or immunizing effects against future uncontrollable stressors (Hannum et al., 1976; Seligman and Maier, 1967; Williams and Maier, 1977).
Resilience-building through exposure to anxiety or distress is not a novel concept, given the many examples of this process in eastern philosophical or religious thinking. For example, Buddhist training (or life style) involves elements of exposure to austere conditions and actively promotes mental control and / or tolerance of suffering. Such resilience training is thought to explain low traumatic stress rates in Tibetan monks subjected to torture (Holtz, 1998).
Examples of austerity training can also observed in the Mevlevi Order of Islamic Sufism, where its new members (i.e. dervishes) undergo, as part of their spiritual training, a 40-day period of solitary confinement in a small enclosed space, living with little food and sleep, and praying. This process, called “çile doldurmak” in Mevlevi terminology, refers to an experience of continuous and prolonged suffering. If someone loses control over the suffering and terminates the 40-day period prematurely, they are expected to start the process all over again. Thus, the idea behind this practice is to help disciples achieve “spiritual maturation” by building up mental and emotional control over anxiety or suffering caused by deprivation of humanly needs. From a psychological point of view, this training technique clearly utilizes the basic principles of CFBT.
Similar resilience-building strategies are also used in the training of soldiers, commandos, special forces, or political activists. For instance, the SERE (Survival, Evasion, Resistance, and Escape) program, used in the training of some military personnel in the United States, involves controlled exposure to ‘torture-like’ procedures to increase resilience against brutal interrogation techniques or torture. The core principle here is the same: by gradually exposing individuals to stressors in a controlled setting, they learn to manage and tolerate distress effectively.
These examples provide valuable insights into how humans cope with extreme stress, what resilience truly means, and how it can be developed. It was indeed such insights that inspired us to shift the focus of behavioral treatment from habituation to strengthening the sense of control. With this background knowledge, it becomes easier to recognize how radically different CFBT is from other psychotherapies that prioritize anxiety reduction. These approaches stem from entirely different philosophical foundations and socio-cultural contexts. It is no accident that methods specifically aimed at fostering resilience originate from Eastern cultures, where poverty, hardship , and suffering have historically been prevalent, in contrast to the affluence and relatively sheltered social environments of Western societies.
Treatment techniques and presumed mechanisms of action
Both exposure treatment and CFBT depend on confronting anxiety-provoking cues to facilitate improvement. However, exposure treatment usually requires prolonged exposure until anxiety decreases or habituation is achieved, whereas CFBT focuses on enhancing the individual’s sense of control over anxiety. While anxiety diminishes with CFBT in most cases, improvement can still occur even without a reduction in anxiety, as the key factor is the increased sense of control. Prolonged exposure is not essential in this approach, as even brief exposures can lead to the desired outcome if they effectively strengthen the individual’s sense of control.
The differing presumed mechanisms of action also influence how the treatment rationale is presented to clients. Exposure treatment emphasizes habituation (e.g., “Your anxiety will decrease if you remain in the feared situation”), while CFBT focuses on building anxiety tolerance and gaining control over its impact on daily life (e.g., “You will learn to tolerate and control your anxiety by facing it and have control over your life again”). As a result, the language used to explain CFBT’s rationale is specifically designed to reduce feelings of helplessness, foster hope and courage, and motivate individuals to confront feared situations. Such effects likely explain the high rates of compliance with treatment and the low rates of dropout in our studies, in contrast to exposure treatments where non-compliance and dropout are common occurrences.
Additionally, the two approaches differ in how they define successful treatment outcomes. In exposure treatment, success is measured by a reduction in anxiety, with the implication that insufficient anxiety reduction would be considered a failure. In contrast, CFBT defines success as the ability to control or tolerate anxiety and free oneself from its debilitating effects on life functioning, regardless of whether anxiety levels are significantly reduced.
While some exposure treatments include both live and imaginal exposure, CFBT focuses exclusively on live exposure. There are several reasons for this singular emphasis on live exposure. First, CFBT was initially developed in post-disaster settings where therapist time had to be used efficiently due to the overwhelming number of individuals seeking help. Second, prior experience indicated that live exposure is a significantly more powerful intervention compared to imaginal exposure, leading to the expectation that live exposure alone would yield sufficient improvement—a prediction later supported by our research findings. Third, CFBT was designed to be suitable for self-administration , enabling its widespread dissemination as a self-help approach to large survivor populations following major disasters. Additionally, minimizing therapist involvement in treatment makes it easier to attribute progress to one’s own efforts rather than to an external agent (Başoğlu et al., 1994), an issue that is critically important in a therapy designed to enhance sense of control.
Therapist involvement in therapy is therefore minimal, as live exposure is self-administered in most cases. The therapist’s role is limited to assessment, explanation of the treatment rationale, teaching clients how to conduct self-exposure, and encouraging self-exposure or prescribing specific instructions, as needed. Additional therapist involvement, such as therapist-assisted exposure and monitoring of progress, is required only in a minority of cases that are not able to initiate self-exposure due to their difficulty in tolerating anxiety.
Treatment procedures
Most trauma therapies highlight the significance of “processing” and “integrating” the trauma narrative as a core element of treatment. The prevailing view is that this focus helps individuals “make sense” of their traumatic experiences, alleviates distress, and fosters healing. This is a cognitive approach to trauma, which is not aligned with the basic principles of CFBT. Cognitive interventions are not needed in CFBT, because cognitive change occurs with improvement in traumatic stress reactions, as demonstrated by our studies. Accordingly, the initial assessment does not necessitate in-depth exploration of the trauma history. While survivors are free to discuss their trauma experiences, they are not urged to delve into specifics. A brief account of the trauma clarifying the nature of the events experienced is sufficient for treatment. Even if the survivor is reluctant to tell the story of their trauma, which may occur in some cases, it does not hinder the treatment process.
CFBT focuses on the survivor’s psychological responses to trauma. A detailed and lengthy psychiatric assessment is not required to obtain the information needed for treatment. Such information is obtained through five self-rated questionnaires: the Screening Instrument for Traumatic Stress, the Depression Rating Scale, the Fear and Avoidance Questionnaire, the Social Disability Scale, and the Global Improvement Scale. These tools, which are also employed regularly during treatment to track progress, provide all the essential data needed for effective therapy. Additionally, using these instruments in treatment augments its impact by offering survivors feedback on their improvement. Such feedback often serves to enhance their sense of control and strengthen their motivation to achieve the goals of treatment.
Traditional exposure therapy typically consists of 8-10 sessions, whereas CFBT does not follow a fixed number of sessions. In our fieldwork with earthquake survivors, most cases required only a single session, with a few additional sessions for those who did not respond initially. As a result, treatment duration varies, usually ranging from 1 to 4 sessions, depending on the individual’s response. In our study (Başoğlu, 2022) of 60 war and torture survivors who had considerably more severe posttraumatic stress reactions than earthquake survivors, the mean number of sessions needed for recovery was 6 (3 or 4 in 20% of the cases, 5 or 6 in 35%, 7 to 10 in 33%, and 12 in 5%). However, it is worth noting that because this study aimed at examining the optimum number of treatment sessions required for much / very much improvement, treatment had to be continued until such improvement occurred. It could have been discontinued earlier, as soon as the survivors showed sufficient reduction in avoidance behaviors (e.g. by 20%), thereby reaching a stage in treatment beyond which they could have conducted exposure on their own. This would have reduced the total number of sessions further. This approach warrants further exploration in future research. Regardless, the key point here is that CFBT employs a flexible treatment duration strategy, making it well-suited for post-disaster field settings where therapist availability and cost-effectiveness are critical considerations.
CFBT also differs from exposure treatments in involving a relatively less structured approach. For example, in Marks and colleagues’ protocol (1998) treatment focuses usually on four main treatment targets that represent the most functionally disabling problems (e.g. ‘to be able to stay alone at home’). Once these targets are defined, then exposure homework tasks are set. Exposure tasks define specific activities that are required to achieve the treatment targets (e.g. ‘To stay alone at home for 2 hours during early evening’). In addition, the clients are asked to keep a diary, regularly recording the executed tasks and rating their anxiety before and after exposure sessions. The diary is then reviewed every week and new tasks are set as treatment progresses. Treatment needs to involve multiple targets, because anxiety reduction in one situation may not necessarily generalize to another.
This approach is not used in CFBT, simply because it does not aim for anxiety reduction in as many feared situations as possible. Hence, it does not involve procedures, such as treatment target setting, monitoring of anxiety during exposure by obtaining within-session anxiety ratings, or diary keeping. Exposure tasks are utilized as a process by which anxiety tolerance and control can be achieved. Treatment usually starts with self-exposure instructions of a general nature (i.e. do not avoid feared situations as you come across them), mainly designed to normalize daily life routines. One or two focused exposure exercises may be considered to maximize treatment impact on sense of control when necessary. Prolonged exposure to anxiety cues is not prescribed, as brief exposures until sense of control develops are deemed sufficient. Exposure can be terminated when sufficient sense of control develops, regardless of the extent of anxiety reduction. Therapist assistance in exposure exercises is considered only when the client is unable to conduct self-exposure due to high levels of anxiety. Exposure treatments often involve fear hierarchy construction (i.e. ordering of exposure tasks from the least to the most anxiety-evoking), whereas in CFBT graduated exposure is used only when a person experiences difficulty in tackling a particular task.
Another key feature that sets CFBT apart from other treatments is its use of both unconditioned stimuli (UCS) and conditioned stimuli (CS) during exposure to anxiety-evoking cues. For instance, earthquake tremors are UCS, and our research has demonstrated that such tremors are the most frightening aspect of earthquakes. In contrast, anxiety-inducing reminders of trauma are considered CS. We have employed an earthquake simulator to expose survivors to UCS, albeit in a simulated form, and observed significantly higher levels of improvement. Similarly, in our study involving war and torture survivors, treatment included exposure to videos depicting war and various forms of interpersonal violence, simulating the original traumatic events (UCS) experienced by the survivors. Some of these events involved extreme traumas, such as torture and gang rape. The degree of improvement seen in this study was also noteworthy. This suggests that exposure to UCS is more effective than exposure to CS, aligning with the theoretical foundation of CFBT.
Although the use of simulated UCS may not be required in most cases, it can be reserved for more severe and challenging cases. As demonstrated by our treatment studies with earthquake survivors that took place during the acute phase of trauma, this unique aspect of CFBT allows it to be effectively applied in ongoing trauma scenarios, where UCS are abundant. In fact, CFBT is likely to achieve even better outcomes in such contexts, particularly in strengthening resilience. Additionally, it is worth noting that among all psychotherapies, CFBT is the only one that is suited for use in such circumstances.
Discussion and concluding remarks
It should be clear from the information provided so far that CFBT is not merely a modified or enhanced version of traditional exposure treatment simply because both involve exposure to anxiety cues. Exposure is, in itself, merely a procedure that lacks inherent therapeutic value unless situated within a meaningful context. If exposure alone were sufficient, incidental encounters with anxiety cues—which are common and unavoidable in everyday life—would naturally lead to recovery from chronic anxiety disorders. We know from the natural progression of anxiety disorders that such unguided exposures often reinforce and perpetuate avoidance behaviors.
Exposure within the framework of CFBT is fundamentally distinct from traditional habituation-based exposure treatments in its theoretical foundations, objectives, rationale, likely mechanisms of action, and specific techniques and procedures. Among these, underlying theory is most important. The essence of a treatment is fundamentally shaped by its underlying theory, as this theory serves as the cornerstone for understanding the etiopathogenesis of a problem and determining the appropriate intervention. This understanding, in turn, guides the treatment’s goals, rationale, and the specific techniques and procedures employed. As explained elsewhere, CFBT originated from learning theory, which posits that anxiety or fear arises from loss of control over traumatic stressors. This implies that regaining control should reverse the traumatic process and this is indeed what CFBT does. The clear association between its underlying theory and its goal, rationale, procedures, and outcome is one of its features that distinguish it from other treatments.
In this connection, one could even argue that current treatments for anxiety are not fundamentally distinct from one another and therefore do not warrant different names. This is because they share the same overarching goal—to reduce anxiety. Although various theories have been advanced to explain how they exert their effects (e.g. “emotional processing,” habituation or extinction of anxiety), this issue still remains unclear. Their differences lie primarily in the specific procedures they employ. Procedures alone do not define a treatment, particularly when they have limited or no therapeutic efficacy. Eye Movement Desensitization and Reprocessing (EMDR) is a case in point. Despite the lack of evidence supporting the therapeutic value of eye movements, EMDR is widely regarded as a distinct treatment, with the term “eye movement” curiously still persisting in its name. Its effects likely stems from imaginal exposure—a relatively weak form of behavioral treatment.
Another example is the distinction between behavioral and cognitive-behavioral treatments. There is no evidence to suggest that cognitive interventions alone, without exposure, are effective. Our studies of CFBT alone clearly demonstrate that cognitive interventions are redundant in treatment. Yet, since the so-called cognitive revolution of the 1990s, cognitive-behavioral treatment has not only maintained its status as the preferred approach for anxiety disorders but has also spawned numerous derivatives, each marketed under different names. This proliferation of labels persists despite the lack of substantive differences in their core mechanisms or outcomes.
One might argue that cognitive and behavioral treatments may also enhance sense of control through anxiety reduction and thus overlap with CFBT in their mechanism of action. There is no compelling evidence to show that these treatments (or any other commonly used psychotherapies) enhance resilience, at least in the way we define resilience (see above). Anxiety can be reduced in many ways, including use of drugs or other chemical substances or psychological strategies such as reliance on safety signals, none of which foster resilience. Resilience-building requires a sharp focus on sense of control, which is lacking in most psychotherapies. Furthermore, the learning that occurs with habituation of anxiety in a particular context often fails to generalize to other contexts, requiring repeated exposures across different scenarios. This can be explained by the limited effects of treatment on sense of control or resilience. Whatever impact these treatments might have on sense of control is likely to be coincidental and thus erratic, incomplete, and unstable.
A significant limitation of habituation-based treatments becomes evident when addressing traumatic stress in ongoing trauma situations, such as during wars or after a catastrophic earthquake followed by numerous aftershocks, where threats to safety persist. Since anxiety or fear is a natural response to life-threatening events, reducing anxiety is not a realistic goal in such contexts. This issue limits the usefulness of traditional treatments, as these situations require an approach focused on building resilience rather than alleviating anxiety. As detailed elsewhere, much of our research on CFBT was conducted with earthquake survivors during the acute phase of trauma, following two major devastating earthquakes in 1999 that occurred three months apart, each followed by hundreds of aftershocks lasting over a year. Despite continued exposure to earthquakes, relapse was extremely rare, highlighting the resilience-enhancing effects of the treatment.
It worth noting here that CFBT is not merely a form of psychotherapy designed exclusively for a limited number of psychiatric conditions. Rather, it is applicable across various aspects of daily life where individuals experience anxiety due to a perceived lack of control. Furthermore, the tools of CFBT extend beyond exposure to anxiety cues. In fact, any intervention that strengthens an individual’s sense of control can serve as a treatment tool. This includes a range of well-known behavioral strategies commonly used to “manage” stress, such as problem-solving techniques, skills training, social skills development, gathering information about problems and potential solutions, seeking emotional support, maintaining predictable daily routines, engaging in creative outlets, breaking tasks into smaller steps, and organizing and prioritizing tasks, among many others. These strategies do not just “manage” stress; they all serve to enhance sense of control. To date, our research on CFBT has primarily focused on traumatic stress reactions, utilizing exposure as a key treatment tool. We have not had a chance to explore its potential in other conditions, which represents a promising avenue for future research.
To conclude this section, CFBT stands apart from other treatments not only in its theoretical foundation but also in its philosophical perspective on the human emotion of anxiety. The emphasis on anxiety reduction as the central aim of therapy reflects a puritanical mindset dominant in Western cultures, where anxiety is viewed as an emotion that must be eradicated to attain human ‘happiness.’ This outlook has become deeply embedded in Western mental healthcare systems, fueling a multi-billion-dollar pharmaceutical industry and a multitude of psychotherapy practices, most of which prioritize reducing anxiety through diverse methods rather than building resilience to cope with it. Anxiety reduction does not necessarily mean increased resilience. Moreover, the pursuit of anxiety reduction also serves a political function by maintaining a specific social order, as it keeps the potentially ‘revolutionary’ nature of anxiety in check. Historically, anxiety or fear has been a catalyst for significant social and political transformations, driving reforms and progress. At the same time, it has been wielded by ruling elites as a tool to subjugate populations. Consider the implications of a society where high levels of resilience render such control over human behavior ineffective—this imaginary scenario highlights the profound societal and political dimensions of the therapeutic focus on anxiety reduction.
References
Başoğlu M (2022) Control-Focused Behavioral Treatment: A brief intervention for survivors of war and torture. Torture, 32, 1-2, 251-263.
Başoğlu, M., Marks, I. M., Kılıç, C., Brewin, C. R. & Swinson, R. P. (1994a). Alprazolam and exposure for panic disorder with agoraphobia. Attribution of improvement to medication predicts subsequent relapse. British Journal of Psychiatry, 164, 652-659.
Başoğlu, M. & Mineka, S. (1992). The role of uncontrollable and unpredictable stress in post-traumatic stress responses in torture survivors. In Torture and its Consequences: Current Treatment Approaches, ed. M. Başoğlu. Cambridge: Cambridge University Press, 182-225.
Başoğlu, M., Mineka, S., Paker, M., Aker, T., Livanou, M. & Gök, S. (1997). Psychological preparedness for trauma as a protective factor in survivors of torture. Psychological Medicine, 27, 1421-1433.
Başoğlu, M., Paker, M., Paker, O., Özmen, E., Marks, I., İncesu, C., Şahin, D. & Sarımurat, N. (1994c). Psychological effects of torture: a comparison of tortured with nontortured political activists in Turkey. American Journal of Psychiatry, 151, 76-81.
Foa, E. B., Hembree, E. A. and Rothbaum, B. O. (2007). Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences (Therapist Guide). New York: Oxford University Press.
Hannum, R., Rosellini, R. and Seligman, M. (1976). Retention of learned helplessness and immunization in the rat from weaning to adulthood. Developmental Psychology, 12, 449–454.
Holtz, T. (1998). Refugee trauma versus torture trauma: A retrospective controlled cohort study of Tibetan refugees. Journal of Nervous and Mental Disease, 186, 24–34.
Marks, I. M., Lovell, K., Noshirvani, H. and Livanou, M. (1998). Treatment of posttraumatic stress disorder by exposure and/or cognitive restructuring: A controlled study. Archives of General Psychiatry, 55, 317–325.
Resick, P. A. and Schnicke, M. K. (1993). Cognitive Processing Therapy for Rape Victims. Newbury Park, CA: Sage.
Seligman, M. E. P. and Maier, S. F. (1967). Failure to escape traumatic shock. Journal of Experimental Psychology: Animal Behavior Processes, 74, 1–9.
Williams, J. and Maier, S. (1977). Transsituational immunisation and therapy of learned helplessness in the rat. Journal of Experimental Psychology: Animal Behavior Processes, 3, 240–252.