CFBT compared with other treatments
Comparison of CFBT with other evidence-based treatments
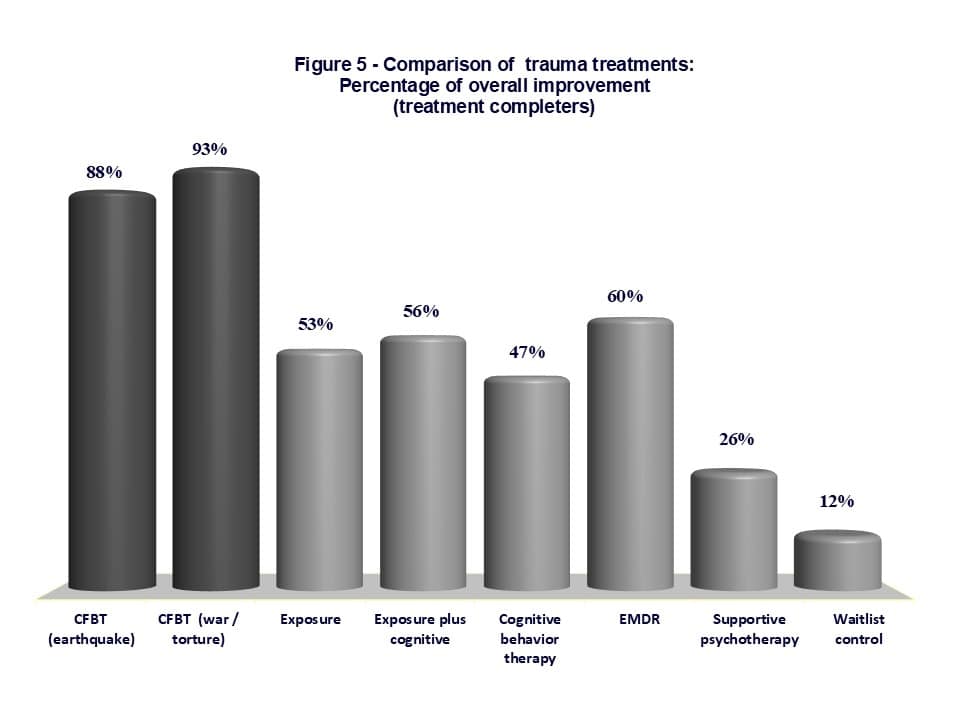 Although comparative studies of CFBT relative to other evidence-based treatments are not available, there is some indirect evidence to suggest that CFBT is superior to other treatments in efficacy. Figure 5 shows a comparison of CFBT (separately for earthquake and war / torture trauma) with other evidence-based treatments in terms of percentage of overall clinical improvement (or responder status). The improvement rate with CFBT in the first group is based on a total of 331 cases from our four treatment studies with earthquake survivors, whereas the improvement rate in the second group is based on 60 treatment completers in our study of CFBT in war and torture survivors (Başoğlu, 2022). These studies are reviewed in the previous section.
Although comparative studies of CFBT relative to other evidence-based treatments are not available, there is some indirect evidence to suggest that CFBT is superior to other treatments in efficacy. Figure 5 shows a comparison of CFBT (separately for earthquake and war / torture trauma) with other evidence-based treatments in terms of percentage of overall clinical improvement (or responder status). The improvement rate with CFBT in the first group is based on a total of 331 cases from our four treatment studies with earthquake survivors, whereas the improvement rate in the second group is based on 60 treatment completers in our study of CFBT in war and torture survivors (Başoğlu, 2022). These studies are reviewed in the previous section.
Figure 5 demonstrates that the global improvement rates observed in our studies are substantially higher than those reported for other treatments. Data for these comparison treatments were sourced from a meta-analysis conducted by Bradley et al (2005), which reviewed 26 studies (totaling 1,535 cases) published between 1980 and 2003. Since meta-analyses of treatment studies seldom report global improvement rates, only one such study was available for comparing treatment outcomes. Notably, more recent meta-analyses, such as that by Cusack et al. (2016)—which analyzed 31 studies conducted between 1980 and 2014—have not found larger between-group effect sizes for these treatments (mean treatment effect sizes across all treatments were 1.32 in Bradley et al. and 1.26 in Cusack et al.). This suggests that the effectiveness of these treatments has not improved over time, even with the inclusion of more recent studies. Therefore, to the extent that the studies included in these meta-analyses reflect current practices, CFBT appears to demonstrate a distinct advantage in effectiveness compared to these other treatments.
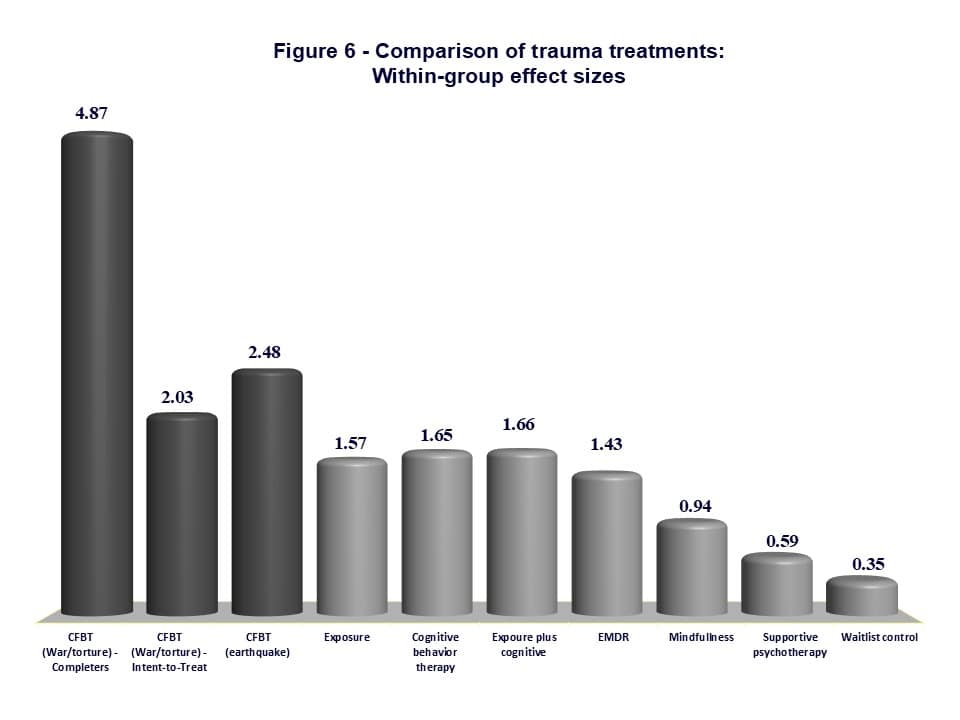 Comparison of between-group effect sizes across treatments is another useful way of comparing different treatments in effectiveness. However, this was only possible using within-group effect size for comparison here, because the pooled sample of 331 cases from our four studies of earthquake survivors included two uncontrolled trials of CFBT (Başoğlu et al, 2003a, 2003b). Again, such data were available only in the Bradley et al study. Figure 6 shows a comparison of treatments in within-group effect sizes. Information of mindfulness-based treatments was obtained from a metanalytical study of Boyd et al (2018) involving treatments such as meditation-relaxation in child survivors of tsunami, mindfulness-based stress reduction, mindfulness-based cognitive therapy or mindfulness-based exposure therapy in war veterans, and mindfulness-based stress reduction in childhood sexual abuse.
Comparison of between-group effect sizes across treatments is another useful way of comparing different treatments in effectiveness. However, this was only possible using within-group effect size for comparison here, because the pooled sample of 331 cases from our four studies of earthquake survivors included two uncontrolled trials of CFBT (Başoğlu et al, 2003a, 2003b). Again, such data were available only in the Bradley et al study. Figure 6 shows a comparison of treatments in within-group effect sizes. Information of mindfulness-based treatments was obtained from a metanalytical study of Boyd et al (2018) involving treatments such as meditation-relaxation in child survivors of tsunami, mindfulness-based stress reduction, mindfulness-based cognitive therapy or mindfulness-based exposure therapy in war veterans, and mindfulness-based stress reduction in childhood sexual abuse.
All within-group effect sizes in Figure 6 were based on Intent-to-Treat analyses, except for the first one (4.87 in war and torture survivors), which is based on completers analysis. This effect size is therefore not comparable with those of other treatments. This information is nonetheless included in the figure to give the reader an idea about the magnitude of pre- to post-treatment change in PTSD symptoms (i.e., treatment efficacy) when survivors complete the treatment process. This finding reflects the substantial reduction in PTSD symptoms (81%-82%), while also explaining the high rate of global improvement (93%) as perceived by the study participants themselves. When the 20 non-completers are included in the analyses the effect size drops to 2.03, which is still substantially greater than the respective figures for other treatments. It is also worth noting here that an effect size of 2.48 in earthquake survivors is achieved by 1 or 2 sessions of CFBT (total session time of 1-2 hours), in comparison with an average of 15.6 total session time in other treatments.
How do these results compare with other studies of war or torture survivors? A similar comparison of CFBT with other evidence-based treatments in asylum seekers or refugees was not possible because most studies do not report global improvement rates (or within-group effect sizes), as noted earlier. However, the results of some studies can be meaningful in this respect. A recent systematic review and meta-analysis (Turrini et al, 2019) of 26 studies involving a total of 1959 participants concluded that “while CBT [Cognitive Behavioral Treatment] was effective in decreasing PTSD and anxiety symptoms, EMDR was effective in terms of depressive symptoms only, and NET [Narrative Exposure Therapy] failed to show a significant effect.” The reported post-treatment between-group effect sizes were 0.71 (1.08 at follow-up) for PTSD symptoms, 1.02 (1.08 at follow-up) for depression, and 1.05 (1.28 at follow-up) for anxiety symptoms. Furthermore, only four studies assessed functioning and quality of life and found no difference between treatments and control conditions (effect size 0.17 for functional disability and 0.23 for quality of life at follow-up). These findings suggest that the so-called trauma-focused treatments do not perform better in asylum-seekers or refugees than in other trauma populations. Although such treatment effects can be statistically significant or effect sizes can be construed as large, there is still substantial room for improvement. Relatively low improvement rates around 50% points to only partial improvement and substantial residual psychopathology implying a serious risk of loss of treatment gains in the long-term.
It is worth illustrating the nature of this problem by examining the results of two studies of NET, a variant of CBT that has gained popularity in treatment of war and torture survivors in recent years. In a controlled study of NET versus Treatment As Usual in asylum-seekers and refugees in Norway, Stenmark et al (2013) reported highly significant treatment effects on PTSD and depression symptoms in the asylum-seeker group with between-group effect sizes of 0.58 and 0.59, respectively. Consistent with such relatively modest effect sizes, 54.5% of the active treatment cases among treatment completers still met the diagnosis of PTSD at 1-month follow-up. Similarly, of the 27 cases with Major Depression before treatment, 16 (59%) still met the diagnosis at the same assessment point. In another study of NET (Hansen et al, 2017) of 110 asylum-seekers and refugees conducted by the Danish Institute Against Torture (DIGNITY) in various North African and Middle Eastern countries, treatment reduced PTSD, anxiety, and depression scores only by 43.7%, 42%, and 28.7%, respectively, with similarly low improvement rates in pain (34.6%) and disability (39%). The authors concluded that these results “strongly suggest that short-term NET therapy can significantly reduce the mental health symptom load of survivors of war and torture.” Some of these results might be statistically significant but the extent of clinical improvement observed unfortunately leaves much to be desired. Clearly, there is still much room for improvement in the efficacy of treatments commonly used with war and torture survivors.
The findings reviewed so far highlight the potency of an intervention that focuses solely on fear and avoidance. It is important to clarify an important issue at this point to avoid a common misunderstanding about CFBT. Therapist-delivered CFBT has three variants: (1) full-course CFBT delivered in 4 to 6 in most cases, (2) single-session CFBT, and (3) single-session CFBT combined with therapist-assisted exposure. The term ‘single-session CFBT’ sometimes leads to the incorrect impression that the improvement achieved by the intervention occurs within the session. When the session does not include therapist-delivered exposure, CFBT is a self-administered intervention and the therapist’s role is limited to explaining the treatment rationale and conveying sufficient sense of control to enhance motivation for treatment. What actually accounts for improvement in traumatic stress in the long term is active efforts on the part of the client after the session (or between sessions, if the treatment involves multiple sessions) to confront feared situations and, consequently, reduced behavioral avoidance. Thus, the initial session merely initiates a self-help process the therapeutic effects of which take about three months to reach a maximum. The following section provides more evidence concerning the self-help element in treatment.
References
Başoğlu M (2022) Control-Focused Behavioral Treatment: A brief intervention for survivors of war and torture. Torture, 32, 1-2, 251-263
Başoğlu, M., Livanou, M. & Şalcıoğlu, E. (2003a). A single session with an earthquake simulator for traumatic stress in earthquake survivors. American Journal of Psychiatry, 160, 788-790.
Başoğlu, M., Livanou, M., Şalcıoğlu, E. & Kalender, D. (2003b). A brief behavioural treatment of chronic post-traumatic stress disorder in earthquake survivors: results from an open clinical trial. Psychological Medicine, 33, 647-654.
Boyd, J.E., Lanius, R.A., & McKinnon, M.C. (2108) Mindfulness-based treatments for posttraumatic stress disorder: a review of the treatment literature and neurobiological evidence. Journal of Psychiatry & Neuroscience,43(1),7–25.
Bradley, R., Greene, J., Russ, E., Dutra, L. & Westen, D. (2005). A multidimensional meta-analysis of psychotherapy for PTSD. American Journal of Psychiatry, 162, 214-227.
Cusack, K., Jonas, D.E., Forneris, C.A., Wines, C., Sonis, J., Middleton, J.C., Feltner, C., Brownley, K.A., Olmsted, K.R., Greenblatt, A., Weil, A., & Gaynes, B.N. (2016) Psychological treatments for adults with posttraumatic stress disorder: A systematic review and meta-analysis. Clinical Psychology Review, 43,128-41.
Hansen, A.K.V., Hansen-Nord, NS., Smeir I., Engelkes-Heby L., & Modvig J. (2017) Impact of Narrative Exposure Therapy on torture survivors in the MENA region. Torture, 27,3,49-63.
Stenmark, H., Catani, C., Neuner, F., Elbert, T., & Holen, A. (2013) Treating PTSD in refugees and asylum seekers within the general health care system. A randomized controlled multicenter study. Behaviour Research and Therapy, 51, 10, 641-647.
Turrini, G., Purgato, M., Acarturk, M. et al (2019) Efficacy and acceptability of psychosocial interventions in asylum seekers and refugees: systematic review and meta-analysis. Epidemiology and Psychiatric Sciences, 1–13.