CFBT in summary
This page includes only a brief overview of Control-Focused Behavioral Treatment (CFBT) and its various applications. More detailed information on various aspects of the treatment can be found in the other sections of this menu.
Theoretical basis of CFBT
Control-Focused Behavioral Treatment (CFBT) is based on learning theory of anxiety, which posits that exposure to unpredictable and uncontrollable stressors is the primary mediating process in traumatic stress (Mineka and Zinbarg, 2006). Its development can be traced back to our work in the early 1990’s when we examined the parallels between animal responses to inescapable shocks and human responses to torture and presented a learning theory formulation of torture trauma (Başoğlu & Mineka, 1992) drawing on the work of Martin Seligman, Steve Maier, Bruce Overmier, Susan Mineka, and other prominent learning theorists and anxiety researchers. Over the years we conducted a series of studies over the years to examine the role of unpredictable and uncontrollable stressors in human responses to war and torture trauma. These studies revealed ample evidence showing that helplessness anxiety or loss of control over threats to safety is indeed strongly associated with traumatic stress. Such evidence implied that traumatic stress can be reversed by interventions that enhance sense of control (or resilience against) traumatic stressors. Hence, CFBT came into existence. It was first tested with earthquake survivors and subsequently with war and torture survivors.
Description
CFBT is an intervention that focuses solely on behavioral avoidance, a common response to traumatic stress. Anxiety and avoidance are hallmark symptoms of trauma (and anxiety disorders), particularly when individuals perceive an ongoing threat to their safety, whether real or imagined. For instance, in the aftermath of an earthquake, the initial catastrophic event is often followed by numerous aftershocks, perpetuating a sense of danger. Similarly, survivors of torture may live with the constant fear of re-arrest or further torture. In such contexts, symptoms like sleep disturbances, hypervigilance, and heightened startle responses to sudden noises or movements are prevalent. Many survivors develop a pervasive fear of situations they associate with potential threat, leading to avoidance behaviors.
 For example, earthquake survivors may avoid entering houses or concrete structures, even when deemed safe, or resist being alone at home, sleeping in the dark, showering, or undressing before bed—activities they associate with vulnerability during an earthquake. Torture survivors, on the other hand, may avoid interactions with military or police personnel, authority figures, or situations reminiscent of their trauma, such as interrogations or medical procedures involving instruments. Additionally, trauma survivors often steer clear of environments or activities that trigger distressing memories of their original trauma. Over time, this avoidance can extend to a broad range of situations, severely impairing social, occupational, and familial functioning.
For example, earthquake survivors may avoid entering houses or concrete structures, even when deemed safe, or resist being alone at home, sleeping in the dark, showering, or undressing before bed—activities they associate with vulnerability during an earthquake. Torture survivors, on the other hand, may avoid interactions with military or police personnel, authority figures, or situations reminiscent of their trauma, such as interrogations or medical procedures involving instruments. Additionally, trauma survivors often steer clear of environments or activities that trigger distressing memories of their original trauma. Over time, this avoidance can extend to a broad range of situations, severely impairing social, occupational, and familial functioning.
Research indicates that 99% of mass trauma survivors experience some form of cognitive or behavioral avoidance, distress in response to trauma reminders, or a combination of both. This generalized fear and avoidance can foster feelings of helplessness, a loss of control over one’s life, and, ultimately, hopelessness and depression. CFBT aims to break this cycle by directly targeting avoidance behaviors, helping survivors regain a sense of control.
When used to treat traumatic stress, CFBT primarily involves exposure to anxiety- or fear cues. It does not involve any of the other techniques commonly used in other treatments. Most importantly, CFBT is distinct from other treatments in not being based on the habituation paradigm, which is central to traditional exposure-based treatments. The primary goal in treatment is to enhance the individual’s sense of control over, or resilience against, anxiety, rather than merely reducing anxiety. While anxiety often diminishes as a person gains a greater sense of control, improvement—as perceived by the individual—can occur even without significant anxiety reduction. (For a discussion of the cause-effect relationship between habituation and sense of control, see mechanisms of recovery.) Consequently, prolonged exposure until habituation occurs is not required; exposure is continued only until the individual develops a sense of control over their anxiety.
The administration of CFBT is described in detail in our 2011 book A Mental Healthcare Model for Mass Trauma Survivors. Briefly, it involves the following procedures:
Step 1: Identify the specific cues that trigger anxiety, fear, or distress,
Step 2: Explain the treatment rationale (i.e., confront your anxiety, fear, or distress until you gain control over it), and
Step 3: Encourage non-avoidance of anxiety- or fear-evoking situation or provide self-exposure instructions.
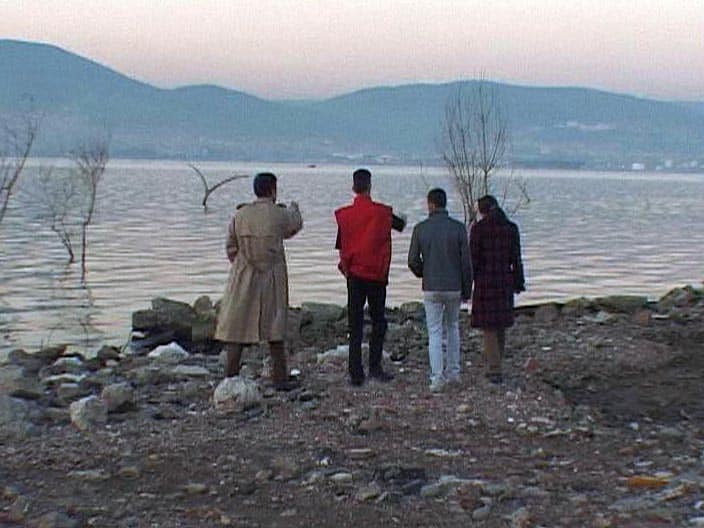
A live exposure session at the disaster site
When used in post-disaster settings, the emphasis of treatment is on self-exposure in the individual’s natural environment without therapist assistance, as this maximizes the treatment’s impact on sense of control. Therapist-assisted exposure, typically limited to just one session, is reserved for cases where the individual has difficulty in initiating or carrying out self-exposure. As such, CFBT is largely rooted in self-help principles. In clinical settings, a full-course version of CFBT involving up to six sessions can be used when necessary.
Explaining the treatment rationale
The way the treatment’s rationale is explained to a person is crucial to its success. Below is an example of a typical narrative that highlights the treatment’s focus on addressing helplessness:
“OK, now that we have clarified how your problems affect your life, let us consider what can be done about them. Fear is your worst enemy here, considering how it affects your life. Instead of fighting and defeating the enemy, you have so far chosen to avoid it. Avoidance means you are surrendering to your fear and letting it take control of your life. This will make you feel totally helpless and hopeless. You will need to take control of your life by confronting your fears and not avoiding situations or activities that make you anxious. So, at this point you have two choices: fight your fear and take control of your life or surrender to it and live your life in fear and feeling helpless. You stand a very good chance of recovery with this treatment. This is entirely your decision, and you will need to take responsibility for it. Which one will it be?”
 This discourse highlights the primary role of anxiety, fear , and associated avoidance or helplessness in traumatic stress. Presenting fear as the enemy, avoidance as surrendering to the enemy, and not avoiding fear as fighting and defeating the enemy serves to enhance sense of control over fear and encourages survivors to relinquish the victim role by taking action against their problem. Presenting a choice between chronic illness and recovery and placing responsibility for this choice squarely on the individual also counters the victim role and enhances motivation for treatment. Note that the ultimate goal of treatment is not presented as freedom from anxiety or fear. The desired outcome is regaining control over stressors and life in general. Informing the individual that the chances of recovery with treatment are high instils hope and alleviates feelings of helplessness and hopelessness (e.g. I will never get better). Our research shows that nearly all individuals recover when they fully comply with treatment.
This discourse highlights the primary role of anxiety, fear , and associated avoidance or helplessness in traumatic stress. Presenting fear as the enemy, avoidance as surrendering to the enemy, and not avoiding fear as fighting and defeating the enemy serves to enhance sense of control over fear and encourages survivors to relinquish the victim role by taking action against their problem. Presenting a choice between chronic illness and recovery and placing responsibility for this choice squarely on the individual also counters the victim role and enhances motivation for treatment. Note that the ultimate goal of treatment is not presented as freedom from anxiety or fear. The desired outcome is regaining control over stressors and life in general. Informing the individual that the chances of recovery with treatment are high instils hope and alleviates feelings of helplessness and hopelessness (e.g. I will never get better). Our research shows that nearly all individuals recover when they fully comply with treatment.
Individuals exposed to mass trauma events of human design, such as wars, political violence, atrocities, and acts of terrorism can easily relate to such discourse, because these terms are not merely allegories relating to fear; they relate to real people perceived as the enemy or perpetrators of human rights abuses. Such discourse is also similar to the one often used in military training of soldiers or in training of political activists. Indeed, using a similar discourse many leaders in history have been able to mobilize masses against a designated enemy and lead them to armed conflicts or wars. Among other examples of this phenomenon are the Kamikaze pilots in World War II, militant political activists, and suicide bombers of today. Such discourse appears to facilitate cognitive control over natural fear of dying and avoidance associated with life-threatening situations.
Combat-related allegories are also helpful in natural disaster survivors, even when used only in reference to fear. This is because people have a natural tendency to personify fear as an adversary and think in terms of fighting, beating, overcoming, defeating, conquering, or winning a victory over fear. Most languages probably have similar expressions, which reflect such a natural tendency in people. In Turkish, for example, “being enslaved by fear” is one the many expressions that describe inability to control fear.
Presenting fear, avoidance, and helplessness as a form of surrender to the ‘enemy’ makes much sense to war survivors, given that much of war violence and gross human rights violations are often designed to terrorize people and force them into total submission and surrender. Such discourse may be particularly helpful in survivors of torture, rape, physical assaults, or other forms of direct victimization, who often have strong feelings of injustice, anger, and desire for vengeance against the perpetrators. These emotions can be channeled into a desire to recover from trauma by helping the survivor see recovery as an act of retribution against or victory over the perpetrators. Survivors of torture, particularly political activists, often relate very well to such suggestions, because they often attribute similar meanings to successful coping with the torture (e.g. not breaking down or submitting to the torturers in any way) and surviving the event in relatively good health. They tend to regard this as their victory over the torturers.
Distinguishing features
CFBT is fundamentally distinct from Cognitive-Behavioral Therapy (CBT) and other exposure-based treatments in its theoretical foundations, objectives, presumed mechanisms of action, and treatment techniques. Its differences from other psychotherapies are reviewed in more detail in the section on distinctive features. Below is a summary of its key distinguishing features:
- A sharp focus on resilience building: CFBT does not rely on the habituation model. Its primary goal is to enhance an individual’s sense of control over or resilience against anxiety, rather than directly reducing anxiety levels. While anxiety often decreases as control increases, meaningful improvement can occur even without significant anxiety reduction. Therefore, prolonged exposure until habituation is achieved is unnecessary; an increased sense of control over anxiety is sufficient. Furthermore, all treatment procedures are designed in ways to maximize treatment impact on the individual’s resilience against anxiety.
- Applicability in high-threat environments: Unlike many psychotherapies that require a safe setting, CFBT can be effectively applied in environments where ongoing threats to safety are unavoidable (e.g., war zones, areas prone to natural disasters). Such settings provide unique opportunities for resilience-building through exposure to unconditioned anxiety stimuli (UCS), which have a more potent effect on resilience than conditioned anxiety stimuli (CS), such as trauma reminders. Even in safe environments, CFBT can incorporate simulated UCS exposures (e.g., simulated earthquake tremors) to achieve therapeutic goals.
- Streamlined treatment procedures: CFBT does not employ common CBT techniques like cognitive restructuring or imaginal exposure. This simplicity makes it easier to administer and train therapists to deliver effectively. Its behavioral focus also enhances its cross-cultural applicability, as it avoids reliance on language-intensive or culturally specific cognitive techniques.
- Emphasis on self-exposure in natural environments: The therapeutic benefits of CFBT primarily stem from self-exposure exercises conducted in the individual’s natural environment. The therapist’s role is often limited to explaining the treatment rationale, encouraging self-exposure, and monitoring progress. This makes CFBT particularly well-suited as a self-help intervention compared to more therapist-dependent treatments.
- Broad range of tools and applications: While exposure is a key component, CFBT is not limited to it. The approach can incorporate any strategy or procedure that enhances an individual’s sense of control over specific stressors or life in general. This flexibility allows CFBT to encompass a wide array of interventions and empowerment strategies, giving it a broader scope and applicability than traditional exposure-based treatments.
As CFBT (Control-Focused Behavioral Treatment) was initially developed through work with earthquake survivors, its application in addressing earthquake-related traumatic stress represents the most advanced and refined form of the treatment. CFBT has several specialized applications or variants tailored specifically to earthquake trauma, including Single-Session CFBT, Earthquake Simulation Treatment, self-administered CFBT using a self-help manual, and full-course CFBT (4 sessions in earthquake survivors, average 6 sessions in war and torture survivors). In post-disaster settings, these applications are often used in combination as part of a broader mental healthcare model. This integrated approach ensures that individuals receive tailored, scalable, and effective interventions based on their specific needs and circumstances, maximizing the potential for recovery and resilience-building in the face of trauma. The studies that led to the development of these applications of CFBT are presented in more detail in Overview of Efficacy.

Single-Session CFBT conducted in groups
In post-disaster circumstances, many survivors may not be able attend treatment more than once, because of disrupted life routines, demographic mobility, and daily struggle for survival. Such circumstances necessitate a single-session treatment that does not require further contact with the client.
Field trials (Başoğlu et al, 2003, 2005) have shown that CFBT can be delivered in a single session to initiate a self-help process (i.e. self-exposure to trauma reminders) resulting in significant clinical improvement in traumatic stress reactions in over 80% of survivors. Such improvement achieved in 3 months was found to have been maintained at 1-2-year follow-up. These findings show that therapist involvement in treatment can be reduced to a minimum and the intervention can be delivered on a largely self-help basis.
Earthquake Simulation Treatment

Earthquake simulator exterior view
Earthquake Simulation Treatment (EST) is designed to help an earthquake survivor gain sense of control over earthquake tremors using an earthquake simulator. It is an innovative treatment developed by DABATEM and used for the first time with earthquake survivors in Turkey. The earthquake simulator is specifically designed for the purposes of CFBT. It is a small furnished house based on a shake table that simulates earthquake tremors up to 8 magnitude on a Richter scale. A computer executes the movements of the simulator in accordance with various preprogrammed earthquake scenarios.

Earthquake simulator interior view
The users can control the tremors from the inside using a mobile control switch, stopping or starting it anytime they want and increasing the intensity whenever they feel ready for it. Being in complete control of the tremors enables users to keep their distress or anxiety within manageable levels. The experience often evokes two types of emotions: fear associated with the tremors and distress related to memories of the traumatic events during the earthquake. This allows opportunities for the users to exercise and gain control over both types of emotions. The session is terminated when the users feel in complete control of their distress or fear. In almost all cases the experience leads to a substantial reduction in these emotions.

Gaining sense of control over tremors in an earthquake simulator
The treatment session usually lasts 45 minutes. About 80% of the session time is spent on the lowest tremor intensity level (3-4 on the Richter scale).
A randomized controlled study (Başoğlu et al, 2007) showed that EST achieves marked improvement in PTSD and depression in 90% of survivors. Improvement generalizes to social, work, and family functioning. In our studies relapse was rare (only 1 case), despite some survivors having been exposed to real earthquakes after treatment, suggesting increased resilience against the traumatic effects of earthquakes.
An imaginative depiction of Earthquake Simulation Treatment – Courtesy of José Carlos Fernandes – a Portuguese artist
EST combined with single-session CFBT achieves 20% more reduction in PTSD than does single-session CFBT alone. Therefore, combined treatment should be the preferred option, whenever an earthquake simulator is available. EST makes subsequent self-exposure easier for survivors who are unable to initiate it by themselves because of high levels of anxiety. Groups of 5 to 10 people could be treated in a single session. This means EST is 50 to 100 times more cost-effective in terms of therapist time, compared to traditional treatments involving 10 sessions per person. Its resilience-building effects suggest that the intervention could also be used in psychologically preparing people against the traumatic effects of future earthquakes in earthquake-prone countries.
Self-help manual

Delivering treatment through a self-help manual
A self-help manual has been developed to facilitate cost-effective treatment dissemination to large numbers of earthquake survivors in the aftermath of major disasters. This is a highly structured manual that can be used as a stand-alone treatment dissemination tool or as an adjunct to therapist-delivered treatment. Its structure closely parallels therapist-delivered treatment. It consists of sections that provide information about traumatic stress symptoms, treatment rationale, self-exposure instructions, target setting, and trouble-shooting at various stages of treatment. The manual includes questionnaires for self-assessment. These questionnaires help the survivor obtain feedback on and monitor progress during treatment.
A pilot study (Başoğlu et al, 2009) suggested that, when delivered after initial therapist contact, about 50% of survivors are likely to improve as much as they do with therapist-delivered treatment. In a further (unpublished) study 1 in 4 survivors utilized the manual and improved when it was disseminated to them without any therapist contact. In our routine fieldwork it was delivered to more than 1,000 survivors with no untoward problems or complications pertaining to self-administered treatment. Audio or video versions of the manual can be used to deliver treatment to illiterate survivors.
Treatment Delivery Manual
 Circumstances after major disasters often require treatment delivery by all means possible. These include mental and other health professionals, general practitioners, nurses, social workers, counselors, schoolteachers, local priests, or other lay people with adequate educational background. The Treatment Delivery Manual is designed to train such people in the delivery of CFBT.
Circumstances after major disasters often require treatment delivery by all means possible. These include mental and other health professionals, general practitioners, nurses, social workers, counselors, schoolteachers, local priests, or other lay people with adequate educational background. The Treatment Delivery Manual is designed to train such people in the delivery of CFBT.
This manual was inspired by our frequent observation that successfully treated survivors often tended to help other family members, friends or neighbors, using the experience they acquired during their own treatment. Sometimes they acted like therapists, encouraging others to conduct self-exposure and even accompanying them into feared situations to help them overcome their fears. In our fieldwork in survivor shelters we actually recruited such survivors as lay therapists and often observed good results. This encouraged us to prepare this manual to facilitate treatment delivery by lay people. The manual is highly structured, guiding the user through all stages of assessment and treatment.
References
Başoğlu M, et al (2003) A brief behavioural treatment of chronic post-traumatic stress disorder in earthquake survivors: Results from an open clinical trial. Psychological Medicine, 33(4): 647-654.
Başoğlu M & Mineka S (1992) The role of uncontrollability and unpredictability of stress in the development of post-torture stress symptoms. In M. Basoglu (Ed.) Torture and Its Consequences: Current Treatment Approaches. Cambridge University Press.
Başoğlu M et al (2011) A mental healthcare model for mass trauma survivors: Control-Focused Behavioral Treatment of earthquake, war, and torture trauma. Cambridge University Press.
Başoğlu M, et al (2005) Single-session behavioral treatment of earthquake-related posttraumatic stress disorder: a randomized waiting list controlled trial. Journal of Traumatic Stress, 18: 1-11.
Başoğlu M, et al (2007) A randomized controlled study of single-session behavioral treatment of earthquake-related posttraumatic stress disorder using an earthquake simulator. Psychological Medicine, 37 (2): 203-214.
Başoğlu M, et al (2009) Single-case experimental studies of a self-help manual for traumatic stress in earthquake survivors. Journal of Behaviour Therapy and Experimental Psychiatry, 40, 50-58.
Mineka S & Zinbarg R (2006). A contemporary learning theory perspective on the etiology of anxiety disorders – It is not what you thought it was. American Psychologist, 61, 10-26.